false
0001526119
0001526119
2025-03-20
2025-03-20
iso4217:USD
xbrli:shares
iso4217:USD
xbrli:shares
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 8-K
CURRENT REPORT
Pursuant to Section 13 or 15(d) of the
Securities Exchange Act of 1934
Date of report (Date of earliest event reported):
March 20, 2025
Verastem,
Inc.
(Exact Name of Registrant as Specified in
Charter)
| Delaware |
|
001-35403 |
|
27-3269467 |
(State or Other Jurisdiction
of Incorporation) |
|
(Commission
File Number) |
|
(IRS Employer
Identification No.) |
| 117 Kendrick Street, Suite 500, Needham, MA |
|
02494 |
| (Address of Principal Executive Offices) |
|
(Zip Code) |
Registrant’s telephone number, including
area code: (781) 292-4200
(Former Name or Former Address, if Changed
Since Last Report)
Check the appropriate box below if the Form 8-K filing is intended
to simultaneously satisfy the filing obligation of the registrant under any of the following provisions:
| ¨ | Written communications pursuant to Rule 425 under
the Securities Act (17 CFR 230.425) |
| ¨ | Soliciting material pursuant to Rule 14a-12 under
the Exchange Act (17 CFR 240.14a-12) |
| ¨ | Pre-commencement communications pursuant to Rule 14d-2(b) under
the Exchange Act (17 CFR 240.14d-2(b)) |
| ¨ | Pre-commencement communications pursuant to Rule 13e-4(c) under
the Exchange Act (17 CFR 240.13e-4(c)) |
Securities registered pursuant to Section 12(b)
of the Act:
| Title of each class |
|
Trading
Symbol(s) |
|
Name
of each exchange on which registered |
| Common stock, $0.0001 par value per share |
|
VSTM |
|
The Nasdaq Capital Market |
Indicate by check mark whether the registrant is an emerging
growth company as defined in Rule 405 of the Securities Act of 1933 (§230.405 of this chapter) or Rule 12b-2 of the Securities
Exchange Act of 1934 (§240.12b-2 of this chapter).
Emerging
growth company ¨
If
an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for
complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ¨
Item 7.01 Regulation FD Disclosure.
On March 20, 2025, Verastem, Inc. posted its updated corporate presentation on
its website, a copy of which is furnished as Exhibit 99.1 to this Current Report on Form 8-K.
Item 9.01 Financial Statements and Exhibits
SIGNATURES
Pursuant to the requirements of the Securities
Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned hereunto duly authorized.
| |
VERASTEM, INC. |
| |
|
|
| Dated:
March 20, 2025 |
By: |
/s/
Daniel W. Paterson |
| |
|
Daniel
W. Paterson |
| |
|
President
and Chief Executive Officer |
Exhibit 99.1
Delivering Novel Therapies for RAS/MAPK Pathway Driven Cancers Corporate Presentation | March 2025
2 Forward - Looking Statements This presentation includes forward - looking statements about, among other things, Verastem Oncology’s (the “Company”) programs and product candidates, strategy, future plans and prospects, including statements relate d to the anticipated timing of a potential launch of avutometinib and defactinib in Low - Grade Serous Ovarian Cancer, the expected outcome and benefits of collaborations, including with GenFleet Therapeutics ( Shanghai), Inc. (GenFleet), including the timing of the IND for VS - 7375 and the initiation of a Phase 1/2a study with respect to the same, the status of enrollments for and potential of the results of the RAM P 301 Phase 3 trial to expand the indication regardless of KRAS mutation status, the structure of our planned and pending cli nic al trials, the potential clinical value of various of the Company's clinical trials, including the RAMP 201, RAMP 205 and RAMP 301 trial s, the timing of commencing and completing trials, including topline data reports, interactions with regulators, the timeline an d indications for clinical development, regulatory submissions, the potential for and timing of commercialization of product ca ndi dates and potential for additional development programs involving the Company’s lead compound and the potential market opportunities of, and estimated addressable markets for, our drug candidates. The words "anticipate," "believe," "estimate," "ex pect," "may," "plan," "target," "potential," "will," "would," "could," "should," "continue," “can” and similar expressions ar e i ntended to identify forward - looking statements, although not all forward - looking statements contain these identifying words. Each forward - l ooking statement is subject to risks and uncertainties that could cause actual results to differ materially from those expres sed or implied in such statement. Applicable risks and uncertainties include the risks and uncertainties, among other things, regarding: the success in the dev elo pment and potential commercialization of our product candidates, including avutometinib in combination with other compounds, including defactinib , LUMAKRAS and others; the uncertainties inherent in research and development, such as negative or unexpected results of clin ica l trials, the occurrence or timing of applications for our product candidates that may be filed with regulatory authorities in any jurisdictions; whether and when regulatory authorities in any jurisdictions may approve any such applicati ons that may be filed for our product candidates, and, if approved, whether our product candidates will be commercially successfu l in such jurisdictions; our ability to obtain, maintain and enforce patent and other intellectual property protection for our pro duc t candidates; the scope, timing, and outcome of any legal proceedings; decisions by regulatory authorities regarding trial de sig n, labeling and other matters that could affect the timing, availability or commercial potential of our product candidates; whet her preclinical testing of our product candidates and preliminary or interim data from clinical trials will be predictive of the re sults or success of ongoing or later clinical trials; that the timing, scope and rate of reimbursement for our product candidates is u nce rtain; that the market opportunities of our drug candidates are based on internal and third - party estimates which may prove to b e incorrect; that third - party payors (including government agencies) may not reimburse; that there may be competitive developments affecting our product candidates; that data may not be available when expected; that enrollment of clinical trials may take l on ger than expected, which may delay our development programs, including delays in review by the FDA of our NDA submission in recur ren t KRAS mutant LGSOC if enrollment in our confirmatory trial is not well underway at the time of submission or that the FDA may require the Company to have completed enrollment or to enroll additional patients in the Company’s ongoing RAMP 301 confi rma tory Phase 3 clinical trial prior to the FDA taking action on our NDA under the accelerated approval pathway; risks associate d with preliminary and interim data, which may not be representative of more mature data, including with respect to interim dur ati on of therapy data; that our product candidates will cause adverse safety events and/or unexpected concerns may arise from additional data or analysis, or result in unmanageable safety profiles as compared to their levels of efficacy; that we may be unable to successfully validate, develop and obtain regulatory approval for companion diagnostic tests for our product candid ate s that require or would commercially benefit from such tests, or experience significant delays in doing so; that the mature RAMP 201 da ta and associated discussions with the FDA may not support the scope of our NDA submission for the avutometinib and defactinib combination in LGSOC, including with respect to KRAS wild type LGSOC; that our product candidates may experience manufacturin g o r supply interruptions or failures; that any of our third - party contract research organizations, contract manufacturing organizations, clinical sites, or contractors, among others, who we rely on fail to fully perform; that we face substantial c omp etition, which may result in others developing or commercializing products before or more successfully than we do which could re sult in reduced market share or market potential for our product candidates; that we will be unable to successfully initiate or compl ete the clinical development and eventual commercialization of our product candidates; that the development and commercializatio n of our product candidates will take longer or cost more than planned, including as a result of conducting additional studies or our decisions regarding execution of such commercialization; that we may not have sufficient cash to fund our contemplated operat io ns, including certain of our product development programs; that we may not attract and retain high quality personnel; that we or Chu gai Pharmaceutical Co., Ltd. will fail to fully perform under the avutometinib license agreement; that our total addressable and target markets for our product candidates might be smaller than we are presently estimating; that we or Secura Bio, Inc. will fail to fully perform under the asset purchase agreement with Secura Bio, Inc., including in relation to milestone payments; that we will not see a return on investment on the payments we have and may continue to make pursuant to the collaboration and option agre eme nt with GenFleet, or that GenFleet will fail to fully perform under the agreement; that we may not be able to establish new o r expand on existing collaborations or partnerships, including with respect to in - licensing of our product candidates, on favorabl e terms, or at all; that we may be unable to obtain adequate financing in the future through product licensing, co - promotional arrangements, public or private equity, debt financing or otherwise; that we will not pursue or submit regulatory filings for ou r product candidates; and that our product candidates may not receive regulatory approval, become commercially successful products, or result in new treatment options being offered to patients. Other risks and uncertainties include those identified under the heading “Risk Factors” in the Company’s Annual Report on For m 1 0 - K for the year ended December 31, 2024 , as filed with the Securities and Exchange Commission (SEC) on March 20 , 2025 , and in any subsequent filings with the SEC, which are available at www.sec.gov and www.verastem.com. The forward - looking statements in this presentation speak only as of the original date of this presentation, and we undertake n o obligation to update or revise any of these statements whether as a result of new information, future events or otherwise, except as required by law. Use of Non - GAAP Financial Measures This presentation contains references to our non - GAAP operating expense, a financial measure that is not calculated in accordanc e with generally accepted accounting principles in the US (GAAP). This non - GAAP financial measure excludes certain amounts or expenses from the corresponding financial measures determined in accordance with GAAP. Management believes this non - GAAP informa tion is useful for investors, taken in conjunction with the Company’s GAAP financial statements, because it provides greater transparency and period - over - period comparability with respect to the Company’s operating performance and can enhance in vestors’ ability to identify operating trends in the Company’s business. Management uses this measure, among other factors, to assess and analyze operational results and trends and to make financial and operational decisions. Non - GAAP information is no t prepared under a comprehensive set of accounting rules and should only be used to supplement an understanding of the Company’s operating results as reported under GAAP, not in isolation or as a substitute for, or superior to, financial inform ati on prepared and presented in accordance with GAAP. In addition, this non - GAAP financial measure is unlikely to be comparable wit h non - GAAP information provided by other companies. The determination of the amounts that are excluded from non - GAAP financial mea sures is a matter of management judgment and depends upon, among other factors, the nature of the underlying expense or income amounts. Reconciliations between this non - GAAP financial measure and the most comparable GAAP financial measure are in cluded in the footnotes to the slides in this presentation on which such non - GAAP number appears. Third - Party Sources Certain information contained in this presentation, including industry and market data and other statistical information, rel ate s to or is based on studies, publications, surveys and other data obtained from third - party sources and the Company’s own intern al estimates and research. While the Company believes these third - party sources to be reliable as of the date of this presentation, it has not independently verified, and makes no representation as to the adequacy, fairness, accuracy or completeness of, any information obtained from third - party sources. In addition, all of the market data included in this presentation involves a numb er of assumptions and limitations, and there can be no guarantee as to the accuracy or reliability of such assumptions Disclaimers
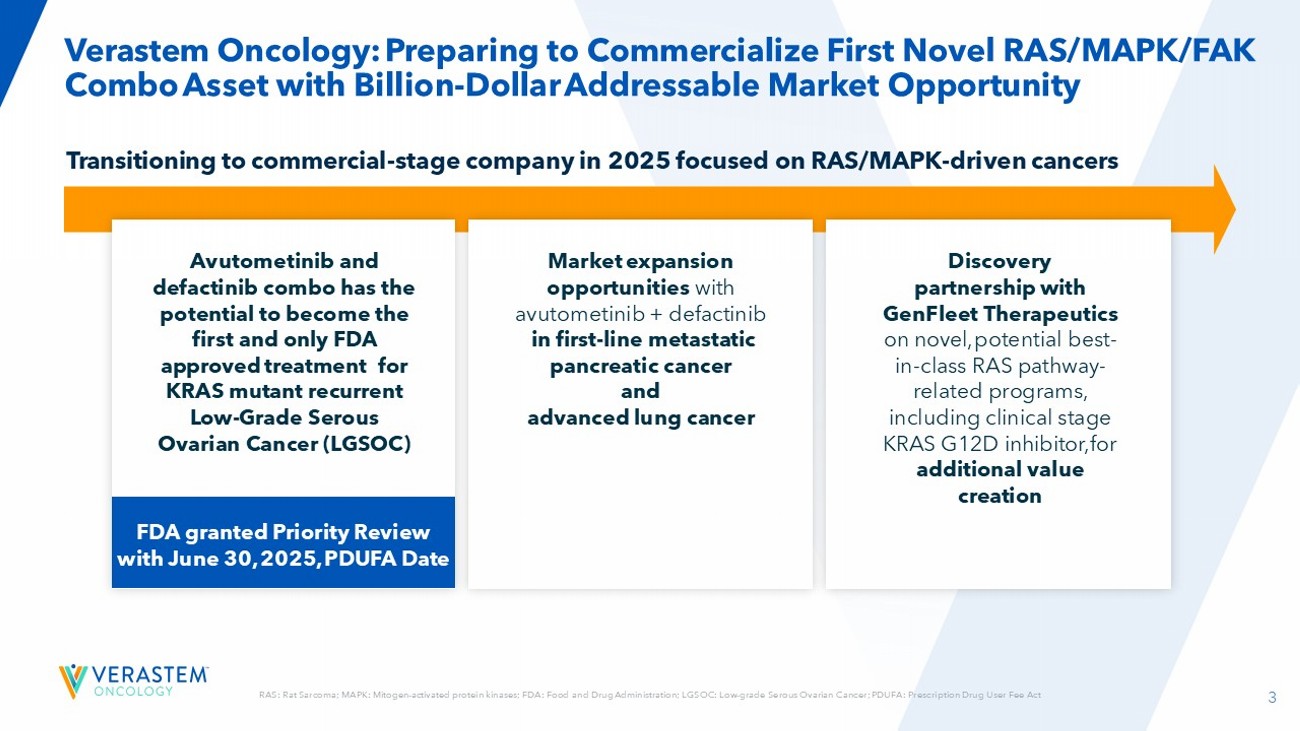
3 RAS: Rat Sarcoma; MAPK: Mitogen - activated protein kinases; FDA: Food and Drug Administration; LGSOC: Low - grade Serous Ovarian Cancer; PDUFA: Prescription Drug User Fee Act Verastem Oncology: Preparing to Commercialize First Novel RAS/MAPK/FAK Combo Asset with Billion - Dollar Addressable Market Opportunity Transitioning to commercial - stage company in 2025 focused on RAS/MAPK - driven cancers Avutometinib and defactinib combo has the potential to become the first and only FDA approved treatment for KRAS mutant recurrent Low - Grade Serous Ovarian Cancer (LGSOC) Discovery partnership with GenFleet Therapeutics on novel, potential best - in - class RAS pathway - related programs, including clinical stage KRAS G12D inhibitor, for additional value creation Market expansion opportunities with avutometinib + defactinib in first - line metastatic pancreatic cancer and advanced lung cancer FDA granted Priority Review with June 30, 2025, PDUFA Date
4 Efficiently Scaled Launch Model to Deliver Best - in - Class Launch for KRAS mutant Recurrent LGSOC in Mid - 2025 Mid - year Launch June 30, 2025 PDUFA Date Potential New Standard of Care Concentrated Launch Focus Significant Market Opportunity Novel/novel combination being reviewed under the Accelerated Approval pathway with Priority Review Avutometinib plus defactinib is differentiated on multiple efficacy measures, favorable tolerability leading to relatively low rates of discontinuation due to AEs Lean and focused field team for access, scientific exchange, and sales Potential high market penetration in KRAS mt recurrent LGSOC in both prevalent and newly recurrent population Surround Sound Support Programs HCO/KEY ACCOUNTS PATIENTS GPO
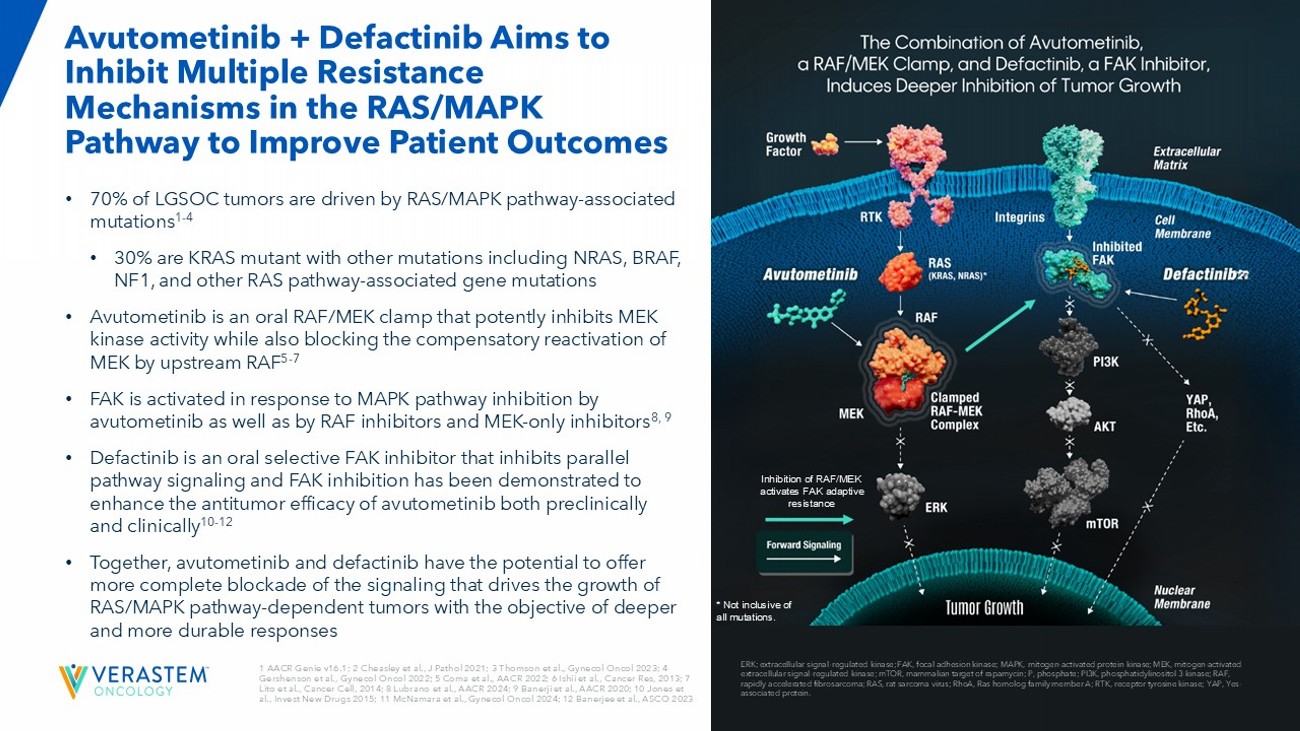
5 1 AACR Genie v16.1; 2 Cheasley et al., J Pathol 2021; 3 Thomson et al., Gynecol Oncol 2023; 4 Gershenson et al., Gynecol Oncol 2022; 5 Coma et al., AACR 2022 ; 6 Ishii et al., Cancer Res, 2013 ; 7 Lito et al., Cancer Cell, 2014 ; 8 Lubrano et al., AACR 2024 ; 9 Banerji et al., AACR 2020 ; 10 Jones et al., Invest New Drugs 2015; 11 McNamara et al., Gynecol Oncol 2024 ; 12 Banerjee et al., ASCO 2023 • 70% of LGSOC tumors are driven by RAS/MAPK pathway - associated mutations 1 - 4 • 30% are KRAS mutant with other mutations including NRAS, BRAF, NF1, and other RAS pathway - associated gene mutations • Avutometinib is an oral RAF/MEK clamp that potently inhibits MEK kinase activity while also blocking the compensatory reactivation of MEK by upstream RAF 5 - 7 • FAK is activated in response to MAPK pathway inhibition by avutometinib as well as by RAF inhibitors and MEK - only inhibitors 8, 9 • Defactinib is an oral selective FAK inhibitor that inhibits parallel pathway signaling and FAK inhibition has been demonstrated to enhance the antitumor efficacy of avutometinib both preclinically and clinically 10 - 12 • Together, avutometinib and defactinib have the potential to offer more complete blockade of the signaling that drives the growth of RAS/MAPK pathway - dependent tumors with the objective of deeper and more durable responses Avutometinib + Defactinib Aims to Inhibit Multiple Resistance Mechanisms in the RAS/MAPK Pathway to Improve Patient Outcomes ERK; extracellular signal - regulated kinase; FAK, focal adhesion kinase; MAPK, mitogen - activated protein kinase ; MEK, mitogen - activated extracellular signal - regulated kinase; mTOR, mammalian target of rapamycin; P, phosphate; PI3K, phosphatidylinositol 3 - kinase; R AF, rapidly accelerated fibrosarcoma; RAS, rat sarcoma virus; RhoA , Ras homolog family member A; RTK, receptor tyrosine kinase; YAP, Yes - associated protein. Inhibition of RAF/MEK activates FAK adaptive resistance * Not inclusive of all mutations.
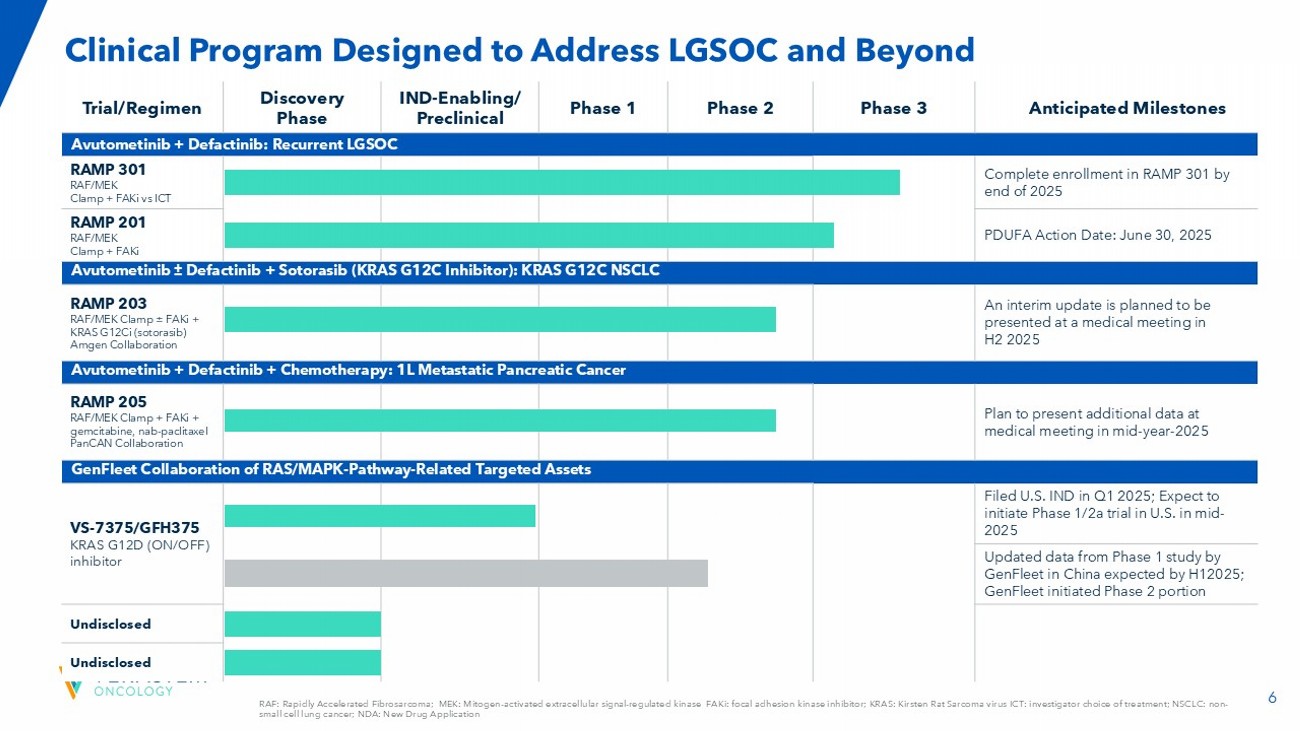
6 Anticipated Milestones Phase 3 Phase 2 Phase 1 IND - Enabling/ Preclinical Discovery Phase Trial/Regimen Avutometinib + Defactinib : Recurrent LGSOC Complete enrollment in RAMP 301 by end of 2025 RAMP 301 RAF/MEK Clamp + FAKi vs ICT PDUFA Action Date: June 30, 2025 RAMP 201 RAF/MEK Clamp + FAKi Avutometinib “ Defactinib + Sotorasib (KRAS G12C Inhibitor): KRAS G12C NSCLC An interim update is planned to be presented at a medical meeting in H2 2025 RAMP 203 RAF/MEK Clamp ± FAKi + KRAS G12Ci (sotorasib) Amgen Collaboration Avutometinib + Defactinib + Chemotherapy: 1L Metastatic Pancreatic Cancer Plan to present additional data at medical meeting in mid - year - 2025 RAMP 205 RAF/MEK Clamp + FAKi + gemcitabine, nab - paclitaxel PanCAN Collaboration GenFleet Collaboration of RAS/MAPK - Pathway - Related Targeted Assets Filed U.S. IND in Q1 2025; Expect to initiate Phase 1/2a trial in U.S. in mid - 2025 VS - 7375/GFH375 KRAS G12D (ON/OFF) inhibitor Updated data from Phase 1 study by GenFleet in China expected by H12025; GenFleet initiated Phase 2 portion Undisclosed Undisclosed RAF: Rapidly Accelerated Fibrosarcoma; MEK: Mitogen - activated extracellular signal - regulated kinase FAKi : focal adhesion kinase inhibitor; KRAS: Kirsten Rat Sarcoma virus ICT: investigator choice of treatment; NSCLC: non - small cell lung cancer; NDA: New Drug Application Clinical Program Designed to Address LGSOC and Beyond
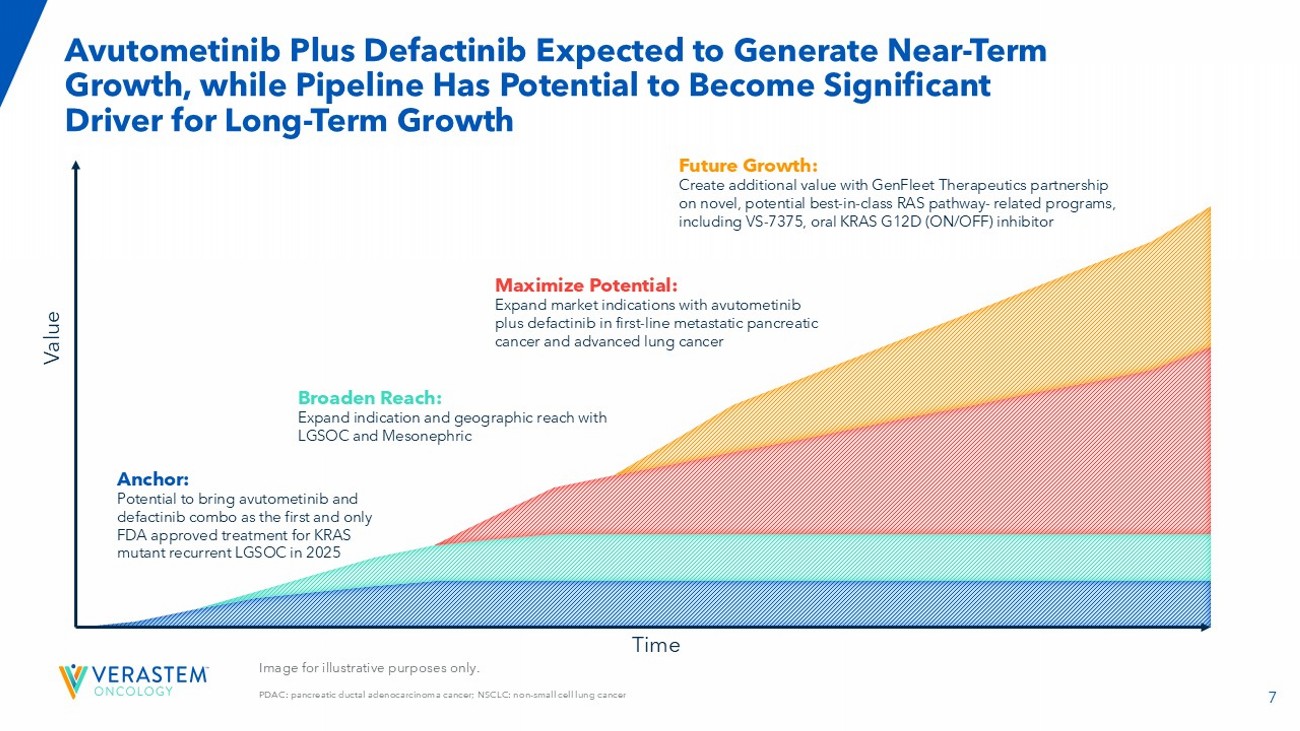
7 Image for illustrative purposes only. PDAC: pancreatic ductal adenocarcinoma cancer; NSCLC: non - small cell lung cancer Avutometinib Plus Defactinib Expected to Generate Near - Term Growth, while Pipeline Has Potential to Become Significant Driver for Long - Term Growth Value Time Anchor: Potential to bring avutometinib and defactinib combo as the first and only FDA approved treatment for KRAS mutant recurrent LGSOC in 2025 Maximize Potential: Expand market indications with avutometinib plus defactinib in first - line metastatic pancreatic cancer and advanced lung cancer Future Growth: Create additional value with GenFleet Therapeutics partnership on novel, potential best - in - class RAS pathway - related programs, including VS - 7375, oral KRAS G12D (ON/OFF) inhibitor Broaden Reach: Expand indication and geographic reach with LGSOC and Mesonephric

Avutometinib and Defactinib in Recurrent Low - Grade Serous Ovarian Cancer (LGSOC) PDUFA Action Date: June 30, 2025 Potential Launch in KRAS mutant Recurrent LGSOC in mid - 2025
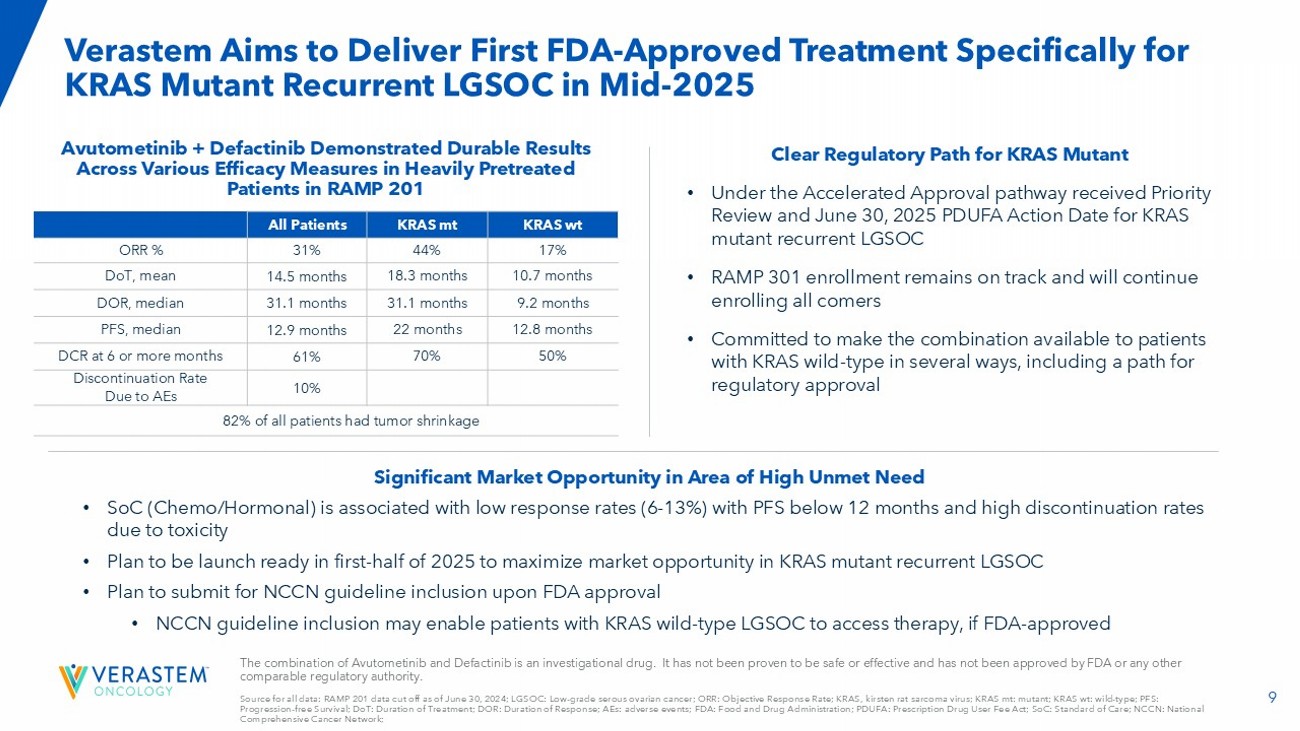
9 Verastem Aims to Deliver First FDA - Approved Treatment Specifically for KRAS Mutant Recurrent LGSOC in Mid - 2025 Avutometinib + Defactinib Demonstrated Durable Results Across Various Efficacy Measures in Heavily Pretreated Patients in RAMP 201 Clear Regulatory Path for KRAS Mutant • Under the Accelerated Approval pathway received Priority Review and June 30, 2025 PDUFA Action Date for KRAS mutant recurrent LGSOC • RAMP 301 enrollment remains on track and will continue enrolling all comers • Committed to make the combination available to patients with KRAS wild - type in several ways, including a path for regulatory approval Significant Market Opportunity in Area of High Unmet Need • SoC (Chemo/Hormonal) is associated with low response rates (6 - 13%) with PFS below 12 months and high discontinuation rates due to toxicity • Plan to be launch ready in first - half of 2025 to maximize market opportunity in KRAS mutant recurrent LGSOC • Plan to submit for NCCN guideline inclusion upon FDA approval • NCCN guideline inclusion may enable patients with KRAS wild - type LGSOC to access therapy, if FDA - approved The combination of Avutometinib and Defactinib is an investigational drug. It has not been proven to be safe or effective and h as not been approved by FDA or any other comparable regulatory authority. Source for all data: RAMP 201 data cut off as of June 30, 2024; LGSOC: Low - grade serous ovarian cancer; ORR: Objective Response Rate; KRAS, kirsten rat sarcoma virus; KRAS mt: mutant; KRAS wt : wild - type; PFS: Progression - free Survival; DoT: Duration of Treatment; DOR: Duration of Response; AEs: adverse events; FDA: Food and Drug Administration; PDUFA: Prescription Drug User Fee Act; SoC: Standard of Care; NCCN: National Comprehensive Cancer Network; KRAS wt KRAS mt All Patients 17% 44% 31% ORR % 10.7 months 18.3 months 14.5 months DoT, mean 9.2 months 31.1 months 31.1 months DOR, median 12.8 months 22 months 12.9 months PFS, median 50% 70% 61% DCR at 6 or more months 10% Discontinuation Rate Due to AEs 82% of all patients had tumor shrinkage
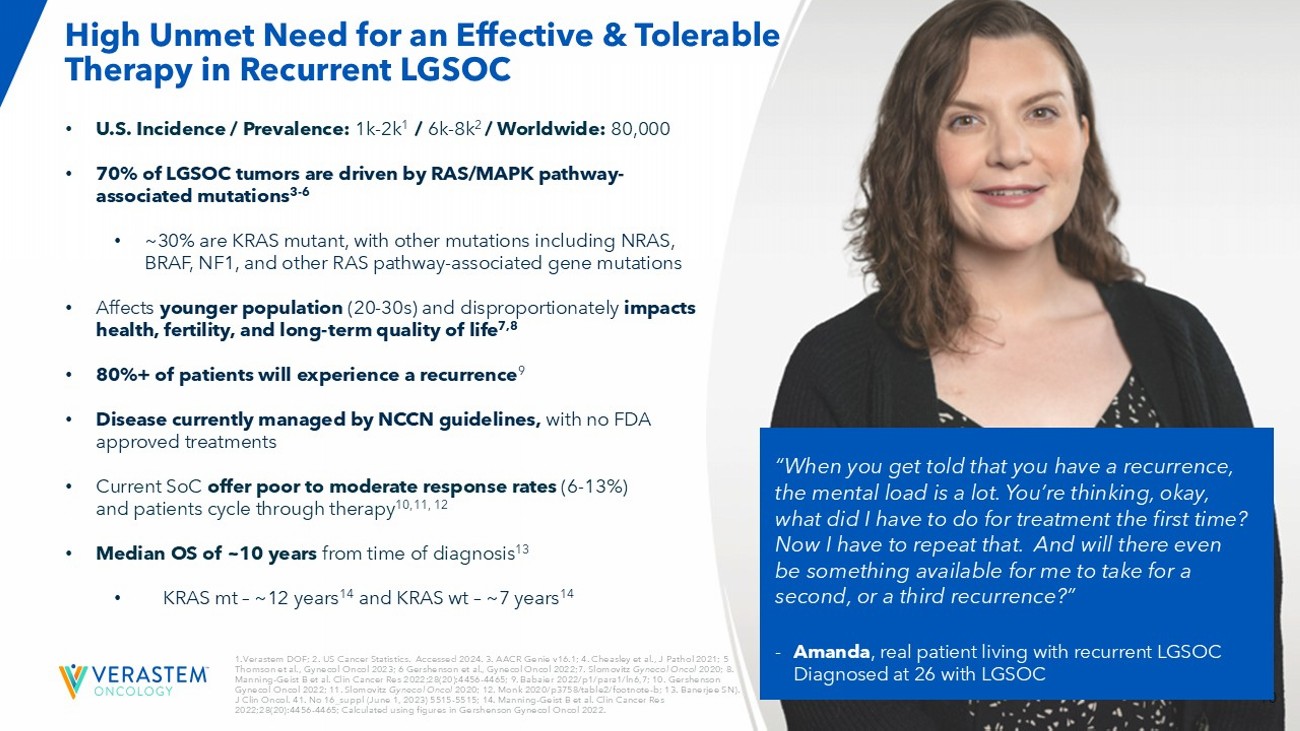
10 “When you get told that you have a recurrence, the mental load is a lot. You’re thinking, okay, what did I have to do for treatment the first time? Now I have to repeat that. And will there even be something available for me to take for a second, or a third recurrence?” - Amanda , real patient living with recurrent LGSOC Diagnosed at 26 with LGSOC High Unmet Need for an Effective & Tolerable Therapy in Recurrent LGSOC • U.S. Incidence / Prevalence: 1k - 2k 1 / 6k - 8k 2 / Worldwide: 80,000 • 70% of LGSOC tumors are driven by RAS/MAPK pathway - associated mutations 3 - 6 • ~30% are KRAS mutant, with other mutations including NRAS, BRAF, NF1, and other RAS pathway - associated gene mutations • Affects younger population (20 - 30s) and disproportionately impacts health, fertility, and long - term quality of life 7,8 • 80%+ of patients will experience a recurrence 9 • Disease currently managed by NCCN guidelines, with no FDA approved treatments • Current SoC offer poor to moderate response rates (6 - 13%) and patients cycle through therapy 10,11, 12 • Median OS of ~10 years from time of diagnosis 13 • KRAS mt – ~12 years 14 and KRAS wt – ~7 years 14 1. Verastem DOF; 2. US Cancer Statistics. Accessed 2024. 3. AACR Genie v16.1; 4. Cheasley et al., J Pathol 2021; 5 Thomson et al., Gynecol Oncol 2023; 6 Gershenson et al., Gynecol Oncol 2022; 7. Slomovitz Gynecol Oncol 2020; 8. Manning - Geist B et al. Clin Cancer Res 2022;28(20):4456 - 4465; 9. Babaier 2022/p1/para1/ln6,7; 10. Gershenson Gynecol Oncol 2022; 11. Slomovitz Gynecol Oncol 2020; 12. Monk 2020/p3758/table2/footnote - b; 13. Banerjee SN). J Clin Oncol. 41. No 16_suppl (June 1, 2023) 5515 - 5515; 14. Manning - Geist B et al. Clin Cancer Res 2022;28(20):4456 - 4465; Calculated using figures in Gershenson Gynecol Oncol 2022.
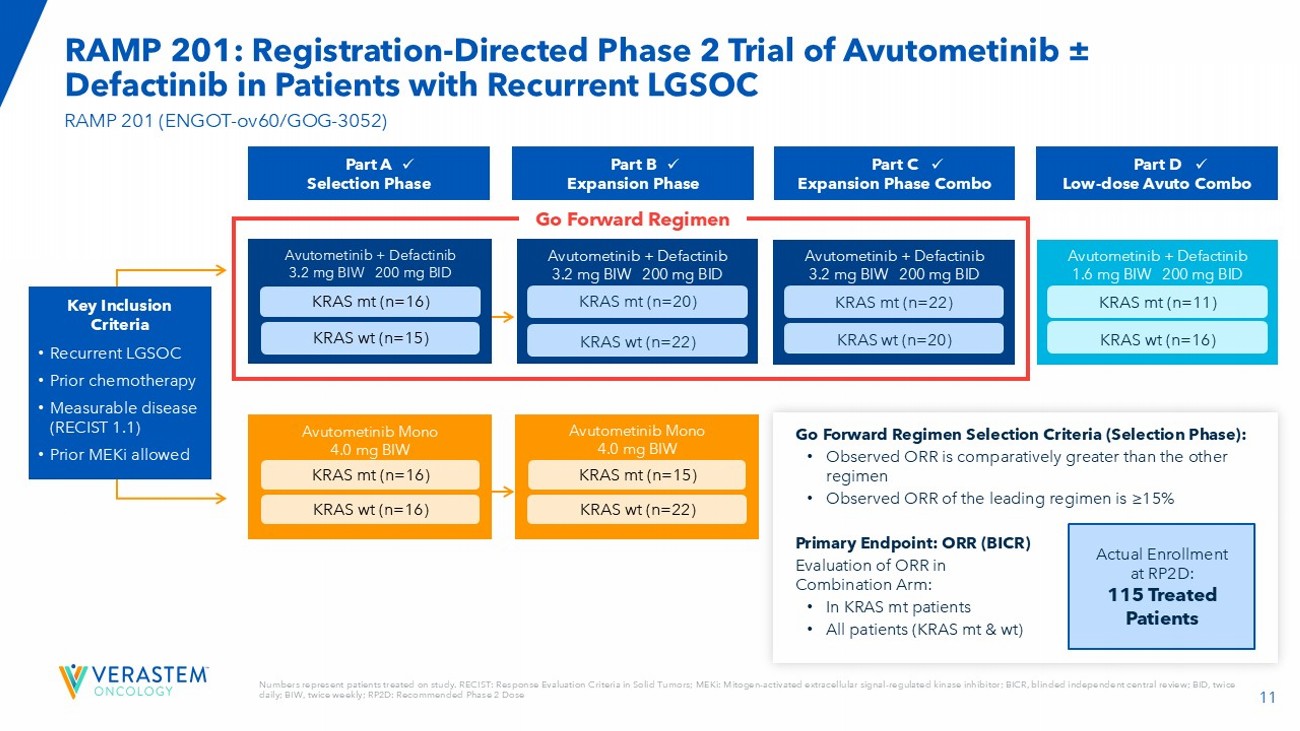
11 Numbers represent patients treated on study. RECIST: Response Evaluation Criteria in Solid Tumors; MEKi : Mitogen - activated extracellular signal - regulated kinase inhibitor; BICR, blinded independent central review; BID, twice daily; BIW, twice weekly; RP2D: Recommended Phase 2 Dose RAMP 201: Registration - Directed Phase 2 Trial of Avutometinib ± Defactinib in Patients with Recurrent LGSOC RAMP 201 (ENGOT - ov60/GOG - 3052) Key Inclusion Criteria • Recurrent LGSOC • Prior chemotherapy • Measurable disease (RECIST 1.1) • Prior MEKi allowed Avutometinib + Defactinib 3.2 mg BIW 200 mg BID KRAS mt (n=20) KRAS wt (n=22) Avutometinib + Defactinib 3.2 mg BIW 200 mg BID KRAS mt (n=22) KRAS wt (n=20) Avutometinib + Defactinib 1.6 mg BIW 200 mg BID Avutometinib + Defactinib 3.2 mg BIW 200 mg BID KRAS mt (n=16) KRAS wt (n=15) Go Forward Regimen Selection Criteria (Selection Phase): • Observed ORR is comparatively greater than the other regimen • Observed ORR of the leading regimen is ≥15% Primary Endpoint: ORR (BICR) Evaluation of ORR in Combination Arm: • In KRAS mt patients • All patients (KRAS mt & wt ) Actual Enrollment at RP2D: 115 Treated Patients Avutometinib Mono 4.0 mg BIW KRAS mt (n=15) KRAS wt (n=22) Avutometinib Mono 4.0 mg BIW KRAS mt (n=16) KRAS wt (n=16) Part A Selection Phase Part B Expansion Phase Part C Expansion Phase Combo Part D Low - dose Avuto Combo x x x x Go Forward Regimen KRAS mt (n=11) KRAS wt (n=16)
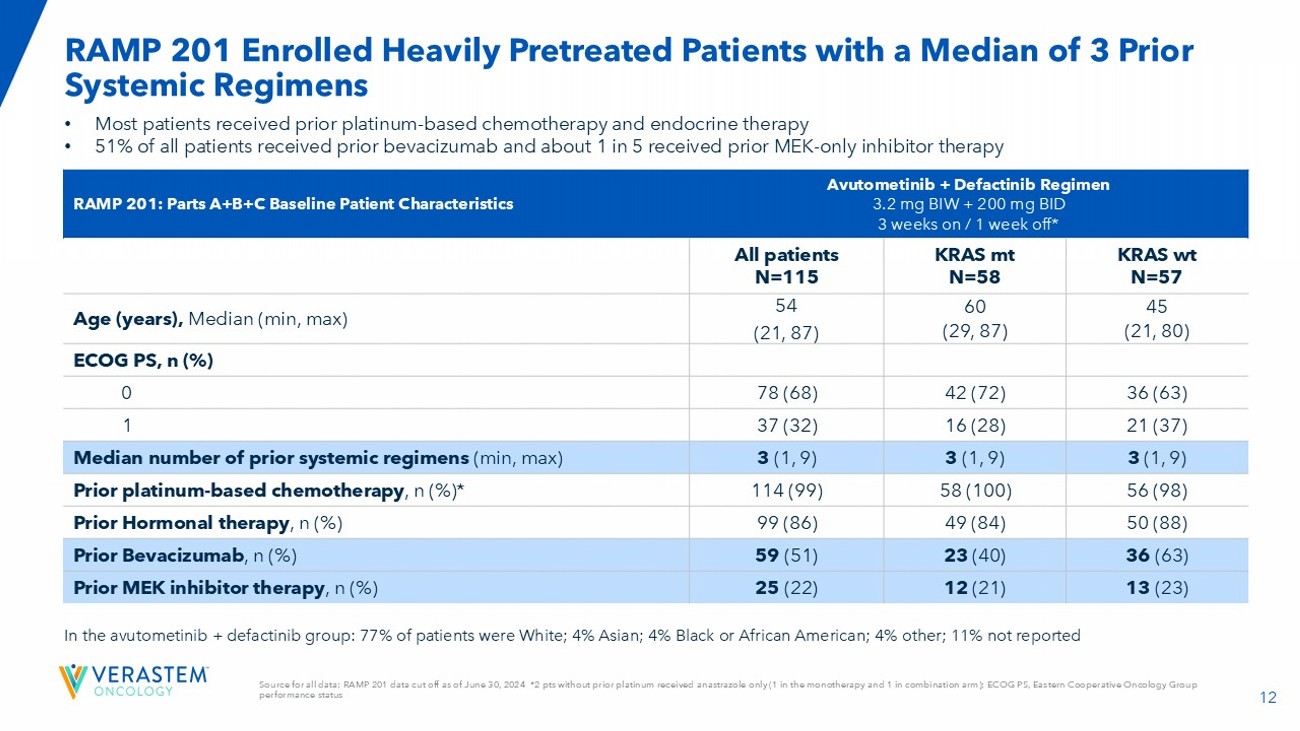
12 Avutometinib + Defactinib Regimen 3.2 mg BIW + 200 mg BID 3 weeks on / 1 week off* RAMP 201: Parts A+B+C Baseline Patient Characteristics KRAS wt N=57 KRAS mt N=58 All patients N=115 45 (21, 80) 60 (29, 87) 54 (21, 87) Age (years), Median (min, max) ECOG PS, n (%) 36 (63) 42 (72) 78 (68) 0 21 (37) 16 (28) 37 (32) 1 3 (1, 9) 3 (1, 9) 3 (1, 9) Median number of prior systemic regimens (min, max) 56 (98) 58 (100) 114 (99) Prior platinum - based chemotherapy , n (%)* 50 (88) 49 (84) 99 (86) Prior Hormonal therapy , n (%) 36 (63) 23 (40) 59 (51) Prior Bevacizumab , n (%) 13 (23) 12 (21) 25 (22) Prior MEK inhibitor therapy , n (%) • Most patients received prior platinum - based chemotherapy and endocrine therapy • 51% of all patients received prior bevacizumab and about 1 in 5 received prior MEK - only inhibitor therapy In th e avutometinib + defactinib group: 77% of patients were White; 4% Asian ; 4% Black or African American; 4% other; 11% not reported Source for all data: RAMP 201 data cut off as of June 30, 2024 *2 pts without prior platinum received anastrazole only (1 in the monotherapy and 1 in combination arm); ECOG PS, Eastern Cooperative Oncology Group performance status RAMP 201 Enrolled Heavily Pretreated Patients with a Median of 3 Prior Systemic Regimens
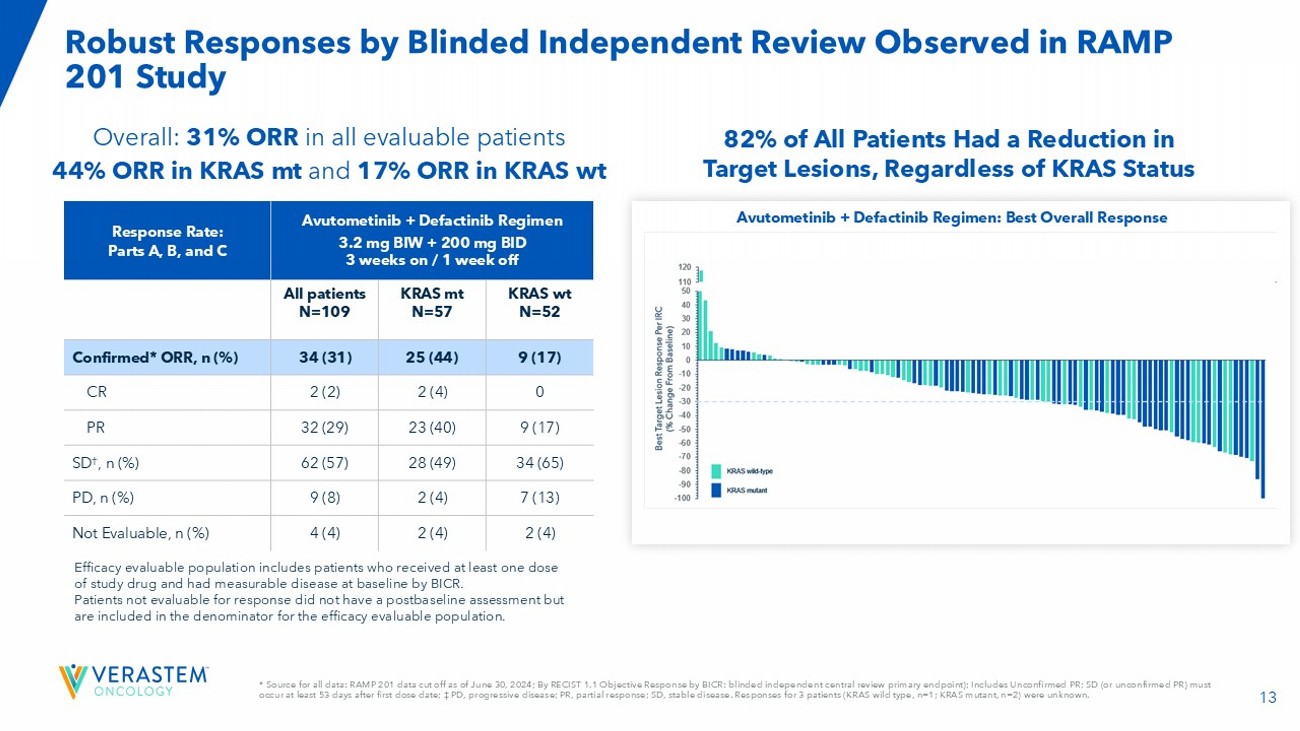
13 Avutometinib + Defactinib Regimen 3.2 mg BIW + 200 mg BID 3 weeks on / 1 week off Response Rate: Parts A, B, and C KRAS wt N=52 KRAS mt N=57 All patients N=109 9 (17) 25 (44) 34 (31) Confirmed* ORR, n (%) 0 2 (4) 2 (2) CR 9 (17) 23 (40) 32 (29) PR 34 (65) 28 (49) 62 (57) SD † , n (%) 7 (13) 2 (4) 9 (8) PD, n (%) 2 (4) 2 (4) 4 (4) Not Evaluable, n (%) Overall: 31% ORR in all evaluable patients 44% ORR in KRAS mt and 17% ORR in KRAS wt Efficacy evaluable population includes patients who received at least one dose of study drug and had measurable disease at baseline by BICR. Patients not evaluable for response did not have a postbaseline assessment but are included in the denominator for the efficacy evaluable population. * Source for all data: RAMP 201 data cut off as of June 30, 2024; By RECIST 1.1 Objective Response by BICR: blinded independe nt central review primary endpoint); Includes Unconfirmed PR; SD (or unconfirmed PR) must occur at least 53 days after first dose date; ‡ PD, progressive disease; PR, partial response; SD, stable disease. Responses for 3 patients (KRAS wild type, n=1; KRAS mutant, n=2) were unknown. Robust Responses by Blinded Independent Review Observed in RAMP 201 Study Avutometinib + Defactinib Regimen: Best Overall Response 82% of All Patients Had a Reduction in Target Lesions, Regardless of KRAS Status
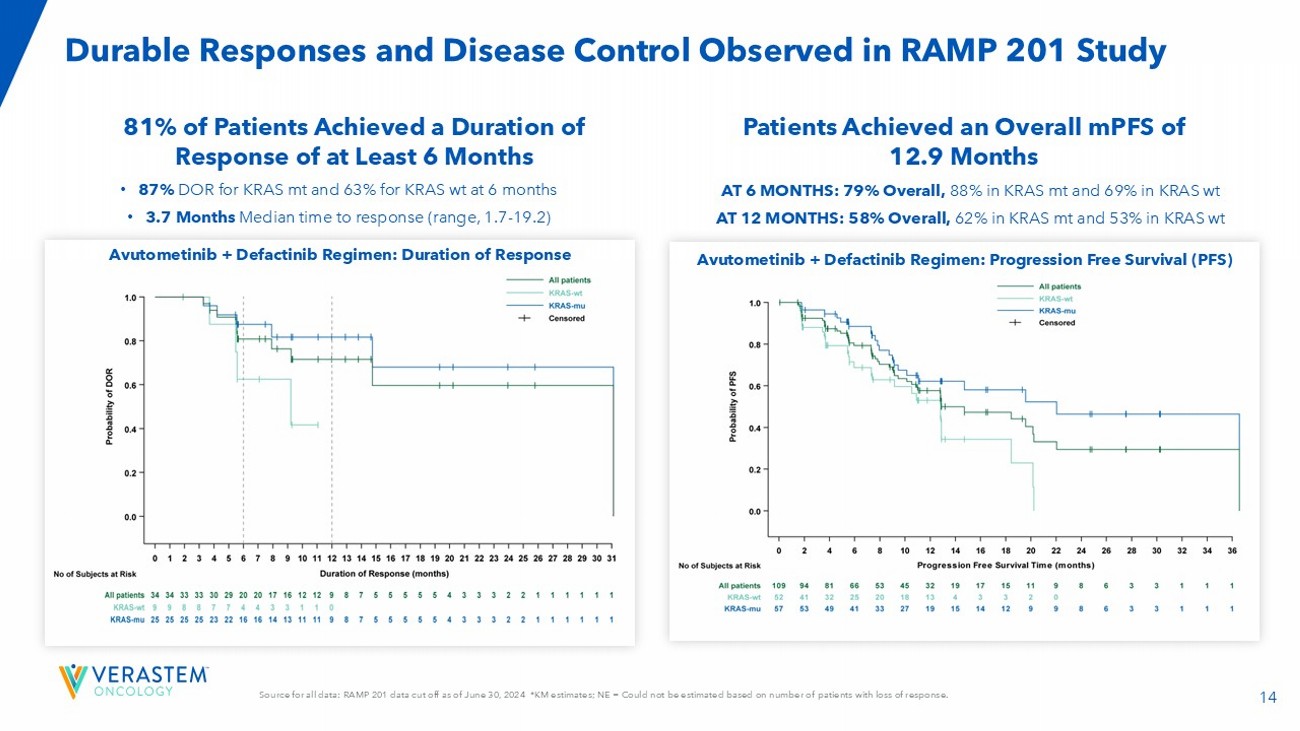
14 Source for all data: RAMP 201 data cut off as of June 30, 2024 *KM estimates; NE = Could not be estimated based on number of pa tients with loss of response. Durable Responses and Disease Control Observed in RAMP 201 Study Avutometinib + Defactinib Regimen: Progression Free Survival (PFS) Avutometinib + Defactinib Regimen: Duration of Response 81% of Patients Achieved a Duration of Response of at Least 6 Months Patients Achieved an Overall mPFS of 12.9 Months • 87% DOR for KRAS mt and 63% for KRAS wt at 6 months • 3.7 Months Median time to response (range, 1.7 - 19.2) AT 6 MONTHS: 79% Overall, 88% in KRAS mt and 69% in KRAS wt AT 12 MONTHS: 58% Overall, 62% in KRAS mt and 53% in KRAS wt
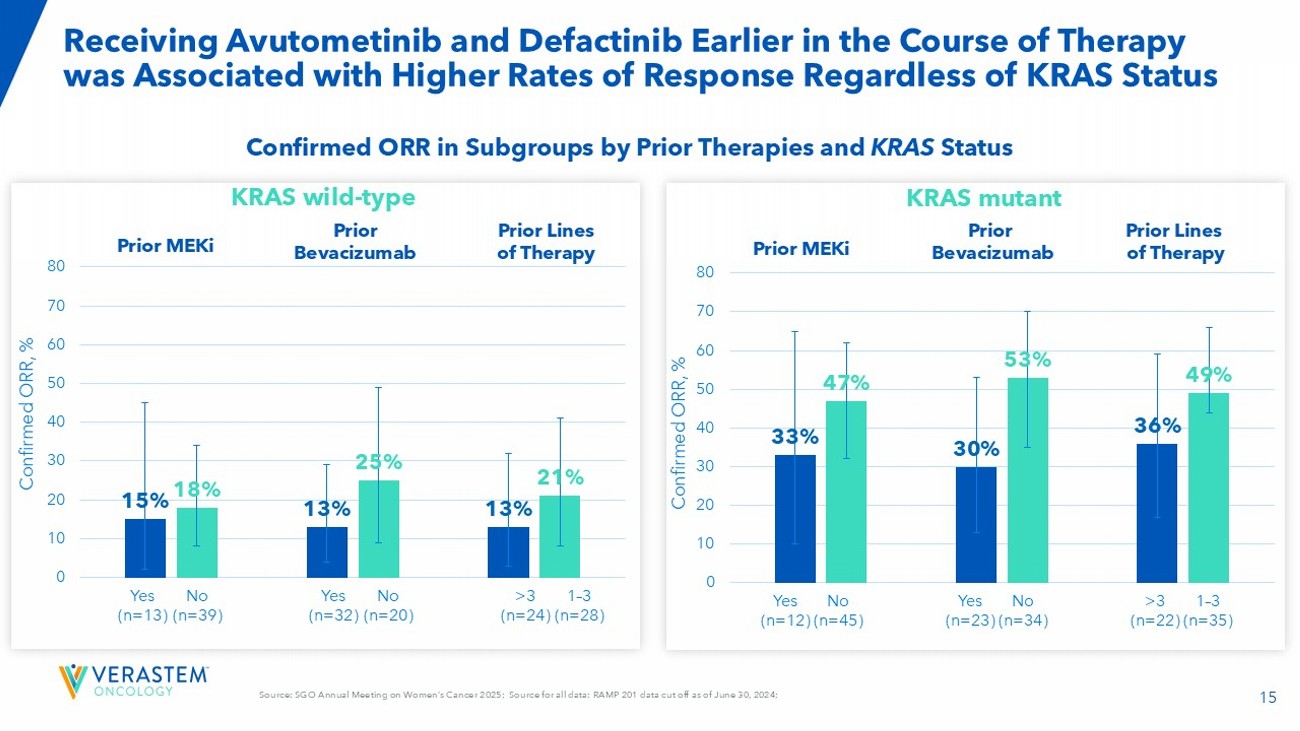
15 Source: SGO Annual Meeting on Women’s Cancer 2025; Source for all data: RAMP 201 data cut off as of June 30, 2024; Receiving Avutometinib and Defactinib Earlier in the Course of Therapy was Associated with Higher Rates of Response Regardless of KRAS Status 15 % 13 % 13 % 18 % 25 % 21 % 0 10 20 30 40 50 60 70 80 Confirmed ORR, % Yes (n=13) No (n=39) Yes (n=32) No (n=20) >3 (n=24) 1 – 3 (n=28) Prior MEKi Prior Bevacizumab Prior Lines of Therapy 33 % 30 % 36 % 47 % 53 % 49 % 0 10 20 30 40 50 60 70 80 Confirmed ORR, % Yes (n=12) No (n=45) Yes (n=23) No (n=34) >3 (n=22) 1 – 3 (n=35) Prior MEKi Prior Bevacizumab Prior Lines of Therapy Confirmed ORR in Subgroups by Prior Therapies and KRAS Status KRAS mutant KRAS wild - type
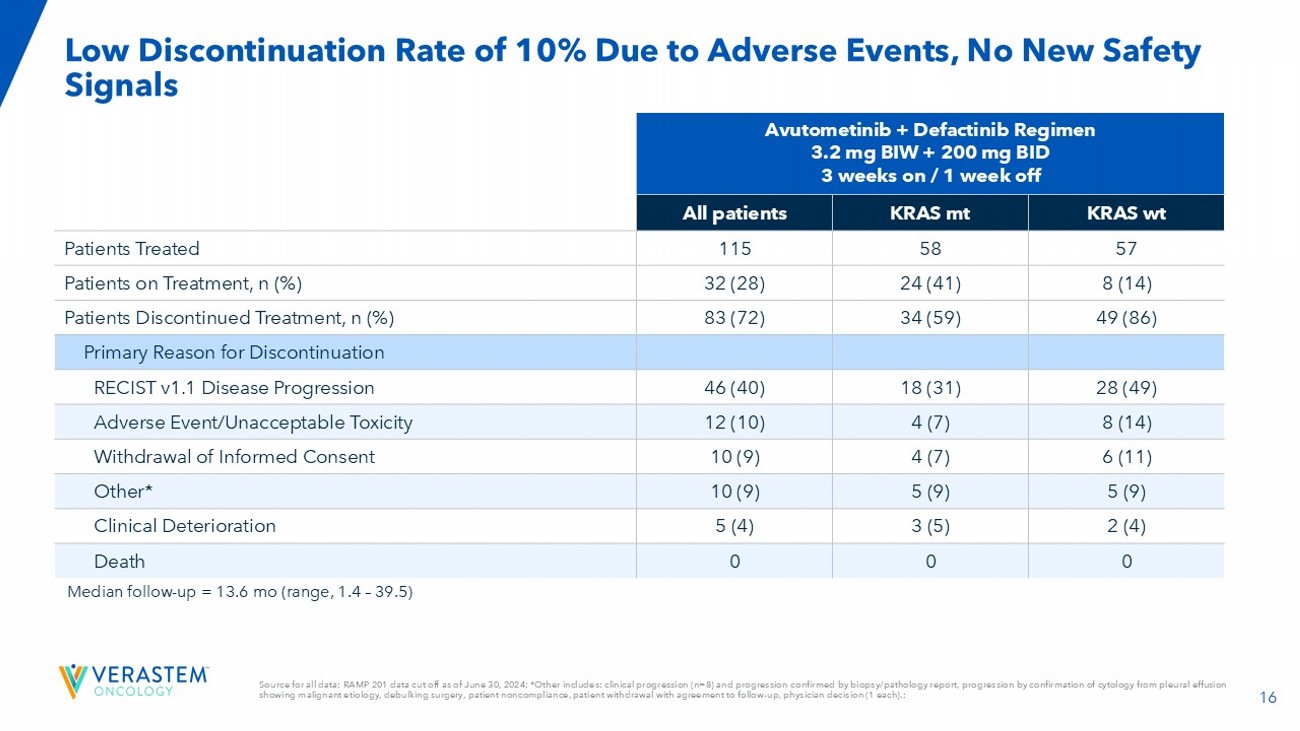
16 Median follow - up = 13.6 mo (range, 1.4 – 39.5) Avutometinib + Defactinib Regimen 3.2 mg BIW + 200 mg BID 3 weeks on / 1 week off KRAS wt KRAS mt All patients 57 58 115 Patients Treated 8 (14) 24 (41) 32 (28) Patients on Treatment, n (%) 49 (86) 34 (59) 83 (72) Patients Discontinued Treatment, n (%) Primary Reason for Discontinuation 28 (49) 18 (31) 46 (40) RECIST v1.1 Disease Progression 8 (14) 4 (7) 12 (10) Adverse Event/Unacceptable Toxicity 6 (11) 4 (7) 10 (9) Withdrawal of Informed Consent 5 (9) 5 (9) 10 (9) Other* 2 (4) 3 (5) 5 (4) Clinical Deterioration 0 0 0 Death Source for all data: RAMP 201 data cut off as of June 30, 2024; *Other includes: clinical progression (n=8) and progression c onf irmed by biopsy/pathology report, progression by confirmation of cytology from pleural effusion showing malignant etiology, debulking surgery, patient noncompliance, patient withdrawal with agreement to follow - up, physician decision (1 each).; Low Discontinuation Rate of 10% Due to Adverse Events, No New Safety Signals
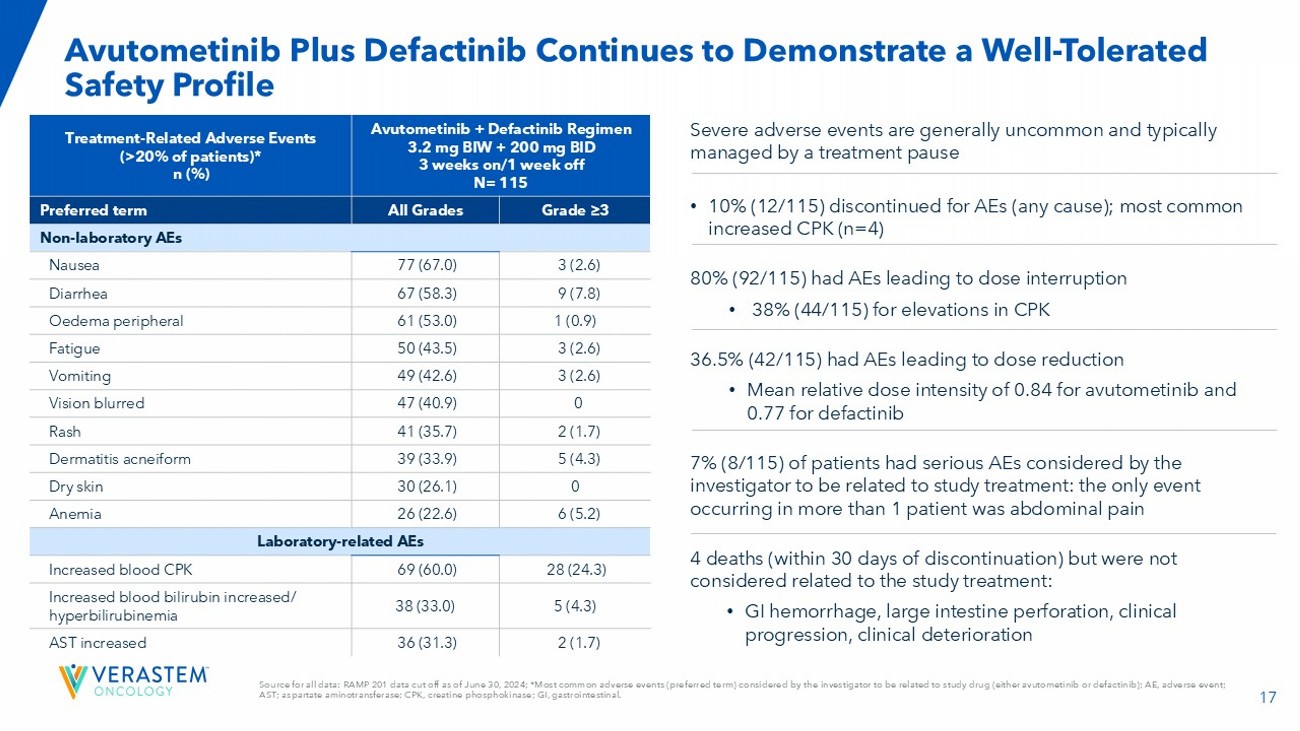
17 Avutometinib + Defactinib Regimen 3.2 mg BIW + 200 mg BID 3 weeks on/1 week off N= 115 Treatment - Related Adverse Events (>20% of patients)* n (%) Grade ≥3 All Grades Preferred term Non - laboratory AEs 3 (2.6) 77 (67.0) Nausea 9 (7.8) 67 (58.3) Diarrhea 1 (0.9) 61 (53.0) Oedema peripheral 3 (2.6) 50 (43.5) Fatigue 3 (2.6) 49 (42.6) Vomiting 0 47 (40.9) Vision blurred 2 (1.7) 41 (35.7) Rash 5 (4.3) 39 (33.9) Dermatitis acneiform 0 30 (26.1) Dry skin 6 (5.2) 26 (22.6) Anemia Laboratory - related AEs 28 (24.3) 69 (60.0) Increased blood CPK 5 (4.3) 38 (33.0) Increased blood bilirubin increased/ hyperbilirubinemia 2 (1.7) 36 (31.3) AST increased Severe adverse events are generally uncommon and typically managed by a treatment pause • 10% (12/115) discontinued for AEs (any cause); most common increased CPK (n=4) 80% (92/115) had AEs leading to dose interruption • 38% (44/115) for elevations in CPK 36.5% (42/115) had AEs leading to dose reduction • Mean relative dose intensity of 0.84 for avutometinib and 0.77 for defactinib 7% (8/115) of patients had serious AEs considered by the investigator to be related to study treatment: the only event occurring in more than 1 patient was abdominal pain 4 deaths (within 30 days of discontinuation) but were not considered related to the study treatment: • GI hemorrhage, large intestine perforation, clinical progression, clinical deterioration Source for all data: RAMP 201 data cut off as of June 30, 2024; *Most common adverse events (preferred term) considered by th e i nvestigator to be related to study drug (either avutometinib or defactinib ); AE, adverse event; AST; aspartate aminotransferase; CPK, creatine phosphokinase; GI, gastrointestinal. Avutometinib Plus Defactinib C ontinues to Demonstrate a W ell - Tolerated Safety Pr ofile
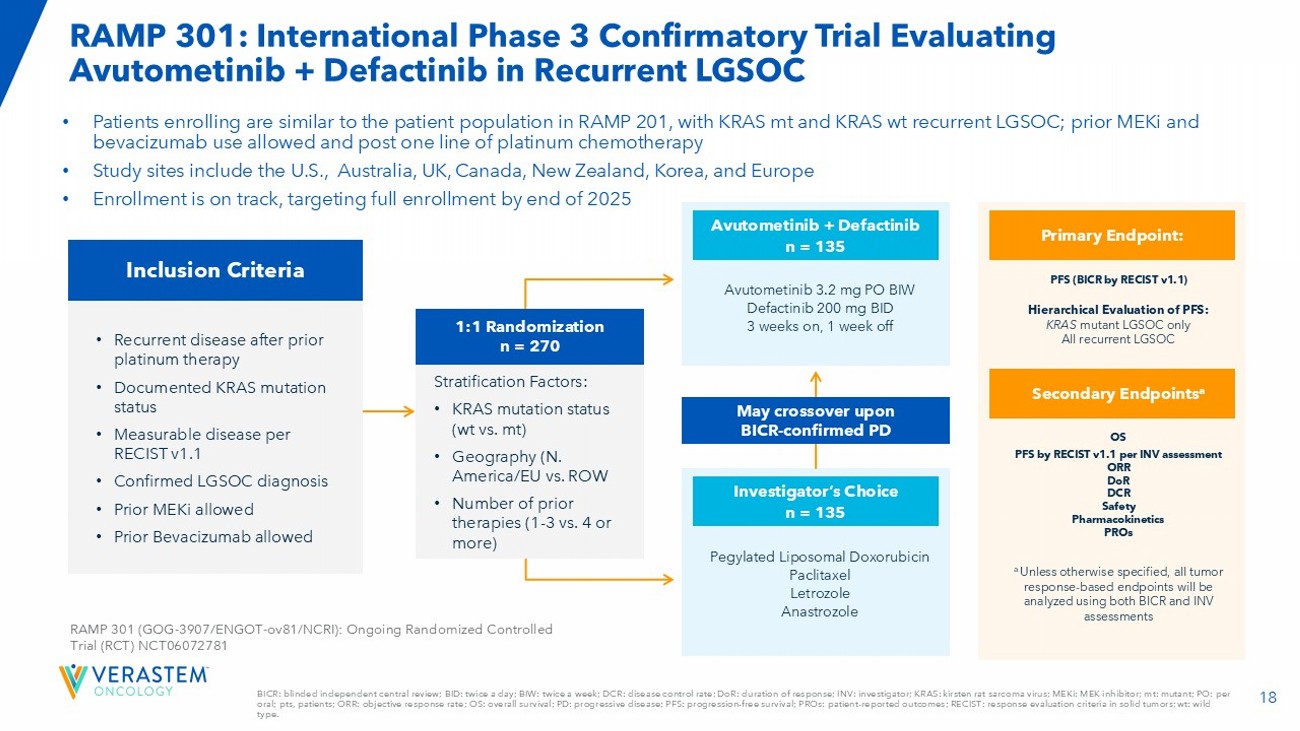
18 BICR: blinded independent central review; BID: twice a day; BIW: twice a week; DCR: disease control rate; DoR : duration of response; INV: investigator; KRAS: kirsten rat sarcoma virus; MEKi : MEK inhibitor; mt: mutant; PO: per oral; pts, patients; ORR: objective response rate; OS: overall survival; PD: progressive disease; PFS: progression - free survival ; PROs: patient - reported outcomes; RECIST: response evaluation criteria in solid tumors; wt : wild type. RAMP 301: International Phase 3 Confirmatory Trial Evaluating Avutometinib + Defactinib in Recurrent LGSOC • Patients enrolling are similar to the patient population in RAMP 201, with KRAS mt and KRAS wt recurrent LGSOC; prior MEKi and bevacizumab use allowed and post one line of platinum chemotherapy • Study sites include the U.S., Australia, UK, Canada, New Zealand, Korea, and Europe • Enrollment is on track, targeting full enrollment by end of 2025 Inclusion Criteria • Recurrent disease after prior platinum therapy • Documented KRAS mutation status • Measurable disease per RECIST v1.1 • Confirmed LGSOC diagnosis • Prior MEKi allowed • Prior Bevacizumab allowed RAMP 301 (GOG - 3907/ENGOT - ov81/NCRI): Ongoing Randomized Controlled Trial (RCT) NCT06072781 Pegylated Liposomal Doxorubicin Paclitaxel Letrozole Anastrozole Investigator’s Choice n = 135 Avutometinib 3.2 mg PO BIW Defactinib 200 mg BID 3 weeks on, 1 week off Avutometinib + Defactinib n = 135 May crossover upon BICR - confirmed PD PFS (BICR by RECIST v1.1) Hierarchical Evaluation of PFS: KRAS mutant LGSOC only All recurrent LGSOC Primary Endpoint: OS PFS by RECIST v1.1 per INV assessment ORR DoR DCR Safety Pharmacokinetics PROs Secondary Endpoints a a Unless otherwise specified, all tumor response - based endpoints will be analyzed using both BICR and INV assessments 1:1 Randomization n = 270 Stratification Factors: • KRAS mutation status ( wt vs. mt) • Geography (N. America/EU vs. ROW • Number of prior therapies (1 - 3 vs. 4 or more)

PDUFA Action Date: June 30, 2025 Potential Launch in KRAS mutant Recurrent LGSOC in mid - 2025 Changing the Treatment Paradigm in Recurrent LGSOC
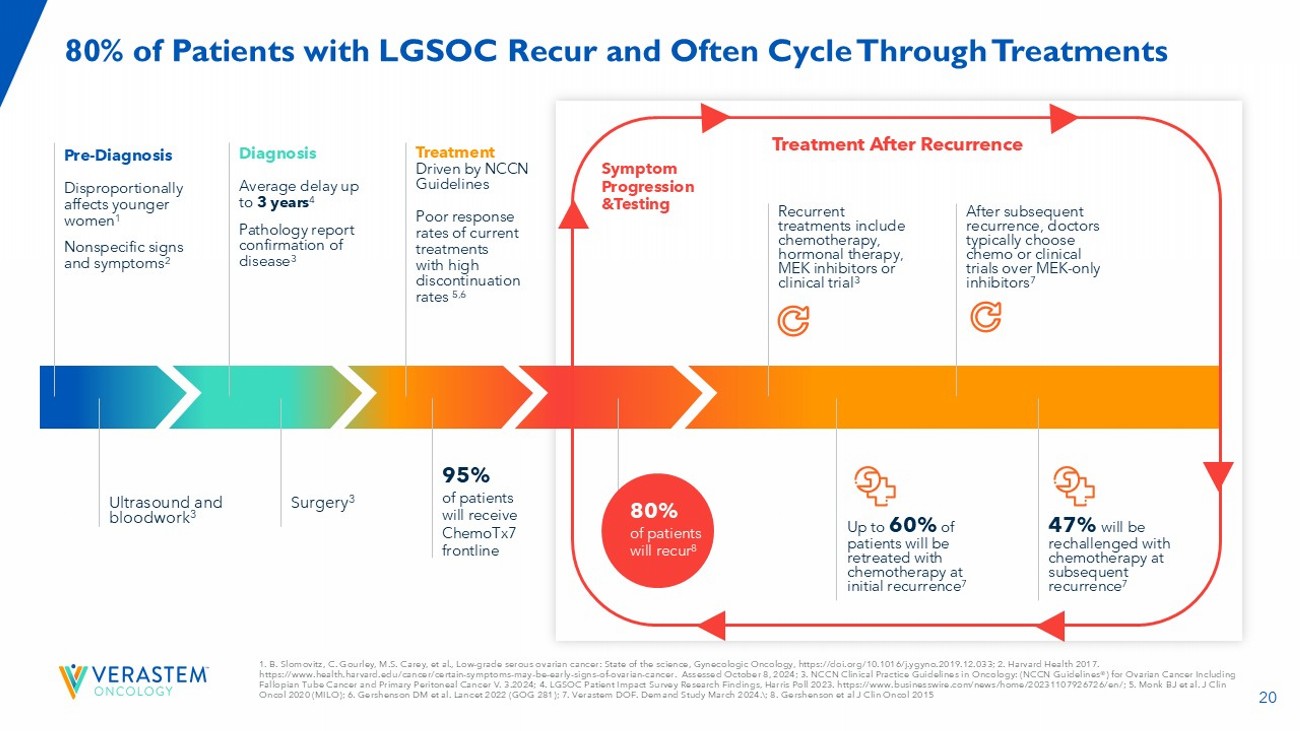
20 Pre - Diagnosis Disproportionally affects younger women 1 Nonspecific signs and symptoms 2 Symptom Progression & Testing Treatment After Recurrence 1. B. Slomovitz , C. Gourley, M.S. Carey, et al., Low - grade serous ovarian cancer: State of the science, Gynecologic Oncology, https:// doi.org /10.1016/j.ygyno.2019.12.033; 2. Harvard Health 2017. https:// www.health.harvard.edu /cancer/certain - symptoms - may - be - early - signs - of - ovarian - cancer. Assessed October 8, 2024; 3. NCCN Clinical Practice Guidelines i n Oncology: (NCCN Guidelines®) for Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer V. 3.2024; 4. LGSOC Patient Impact Survey Research Findings, Harris Poll 202 3. https:// www.businesswire.com /news/home/20231107926726/ en /; 5. Monk BJ et al. J Clin Oncol 2020 (MILO); 6. Gershenson DM et al. Lancet 2022 (GOG 281); 7. Verastem DOF. Demand Study March 2024. ; 8. Gershenson et al J Clin Oncol 2015 80% of Patients with LGSOC Recur and Often Cycle Through Treatments Diagnosis Average delay up to 3 years 4 Pathology report confirmation of disease 3 Treatment Driven by NCCN Guidelines Poor r esponse rates of current treatments w ith high discontinuation rates 5,6 Ultrasound and bloodwork 3 Surgery 3 95% of patients will receive ChemoTx7 frontline Recurrent treatments include chemotherapy, hormonal therapy, MEK inhibitors or clinical trial 3 After subsequent recurrence, doctors typically choose chemo or clinical trials over MEK - only inhibitors 7 Up to 60% of patients will be retreated with chemotherapy at initial recurrence 7 47% will be rechallenged with chemotherapy at subsequent recurrence 7 &UHDWHG E 5DQDK 3L[HO 6WXGLR IURP WKH 1RXQ 3URMHFW 80% of patients will recur 8
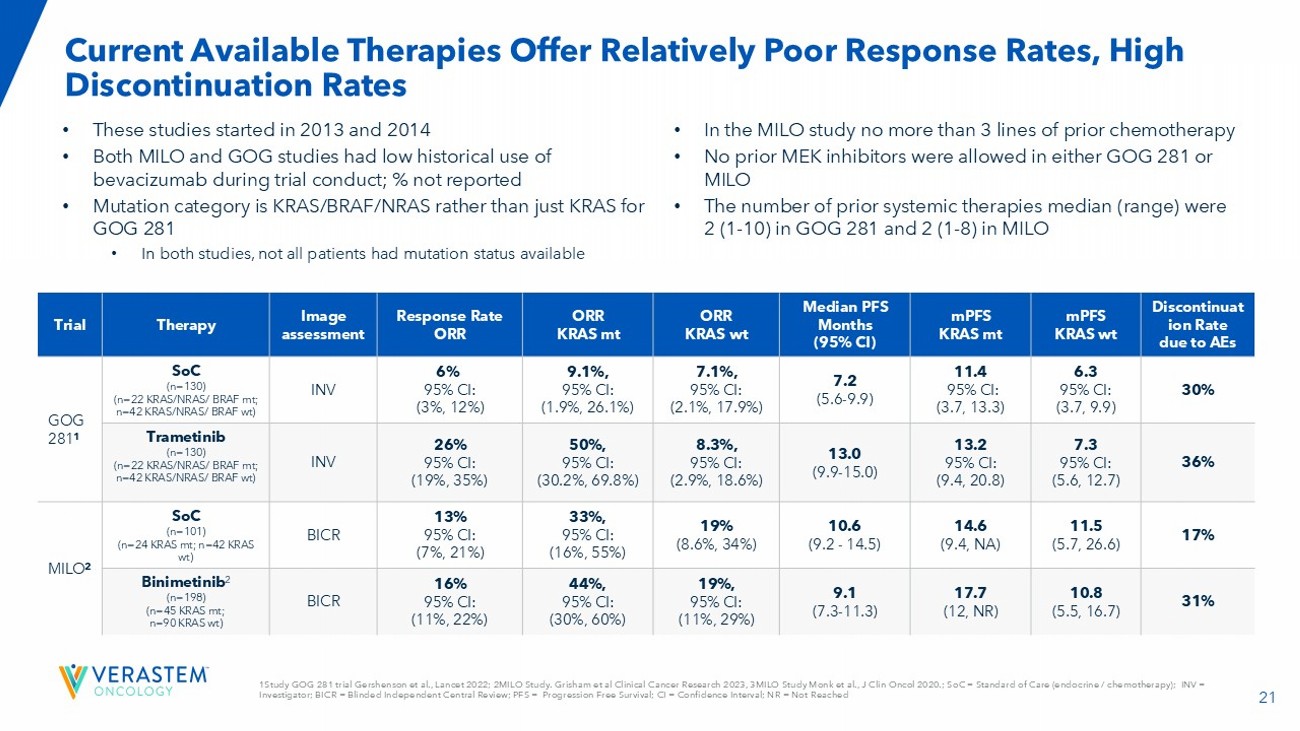
21 1Study GOG 281 trial Gershenson et al., Lancet 2022; 2MILO Study. Grisham et al Clinical Cancer Research 2023, 3MILO Study Monk et al., J Clin Oncol 2020.; S oC = Standard of Care (endocrine / chemotherapy); INV = Investigator; BICR = Blinded Independent Central Review; PFS = Progression Free Survival; CI = Confidence Interval; NR = Not Re ached Current Available Therapies Offer Relatively Poor Response Rates, High Discontinuation Rates • These studies started in 2013 and 2014 • Both MILO and GOG studies had low historical use of bevacizumab during trial conduct; % not reported • Mutation category is KRAS/BRAF/NRAS rather than just KRAS for GOG 281 • In both studies, n ot all patients had mutation status available • In the MILO study no more than 3 lines of prior chemotherapy • No prior MEK inhibitors were allowed in either GOG 281 or MILO • The number of prior systemic therapies median (range) were 2 (1 - 10) in GOG 281 and 2 (1 - 8) in MILO Discontinuat ion Rate due to AEs mPFS KRAS wt mPFS KRAS mt Median PFS Months (95% CI) ORR KRAS wt ORR KRAS mt Response Rate ORR Image assessment Therapy Trial 30% 6.3 95% CI: (3.7, 9.9) 11.4 95% CI: (3.7, 13.3) 7.2 (5.6 - 9.9) 7.1%, 95% CI: (2.1%, 17.9%) 9.1%, 95% CI: (1.9%, 26.1%) 6% 95% CI: (3%, 12%) INV SoC (n=130) (n=22 KRAS/NRAS/ BRAF mt; n=42 KRAS/NRAS/ BRAF wt ) GOG 281 1 36% 7.3 95% CI: (5.6, 12.7) 13.2 95% CI: (9.4, 20.8) 13.0 (9.9 - 15.0) 8.3%, 95% CI: (2.9%, 18.6%) 50%, 95% CI: (30.2%, 69.8%) 26% 95% CI: (19%, 35%) INV Trametinib (n=130) (n=22 KRAS/NRAS/ BRAF mt; n=42 KRAS/NRAS/ BRAF wt ) 17% 11.5 (5.7, 26.6) 14.6 (9.4, NA) 10.6 (9.2 - 14.5) 19% (8.6%, 34%) 33%, 95% CI: (16%, 55%) 13% 95% CI: (7%, 21%) BICR SoC (n=101) (n=24 KRAS mt; n=42 KRAS wt ) MILO 2 31% 10.8 (5.5, 16.7) 17.7 (12, NR) 9.1 (7.3 - 11.3) 19%, 95% CI: (11%, 29%) 44%, 95% CI: (30%, 60%) 16% 95% CI: (11%, 22%) BICR Binimetinib 2 (n=198) (n=45 KRAS mt; n=90 KRAS wt )
22 1Data from RAMP 201 study June 30. 2024 cutoff; 2Chenard - Poirier, et al. ASCO 2017; References: Banerji, Q4 2020 report Avutometinib + Defactinib Combo Has the Potential to Address Key Treatment Needs To date, avutometinib + defactinib combination data in recurrent LGSOC show 1 : Long progression - free survival and duration of treatment Low discontinuation rates due to adverse events Favorable tolerability profile, supported by novel intermittent dosing schedule, with oral treatments 2 Clinically meaningful response rates and durable benefit in both KRAS mutant and wild - type tumors
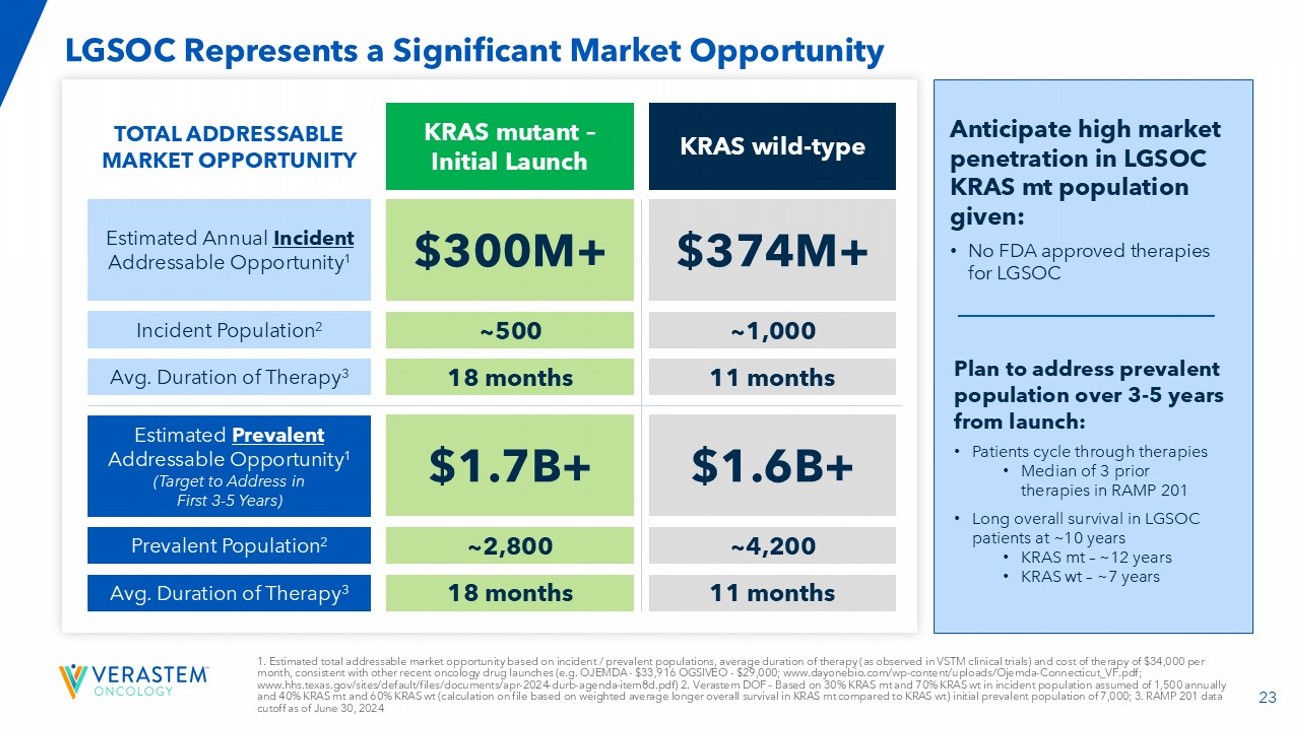
23 1. Estimated total addressable market opportunity based on incident / prevalent populations, average duration of therapy (as obs erved in VSTM clinical trials) and cost of therapy of $34,000 per month, consistent with other recent oncology drug launches (e.g. OJEMDA - $33,916 OGSIVEO - $29,000; www.dayonebio.com/wp - conten t/uploads/Ojemda - Connecticut_VF.pdf; www.hhs.texas.gov/sites/default/files/documents/apr - 2024 - durb - agenda - item8d.pdf) 2. Verastem DOF – Based on 30% KRAS mt and 70% KRAS wt in incident population assumed of 1,500 annually and 40% KRAS mt and 60% KRAS wt (calculation on file based on weighted average longer overall survival in KRAS mt compared to KRAS wt ) initial prevalent population of 7,000; 3. RAMP 201 data cutoff as of June 30, 2024 LGSOC Represents a Significant Market Opportunity KRAS mutant – Initial Launch KRAS wild - type Estimated Prevalent Addressable Opportunity 1 (Target to Address in First 3 - 5 Years) Prevalent Population 2 Avg. Duration of Therapy 3 Estimated Annual Incident Addressable Opportunity 1 Incident Population 2 Avg. Duration of Therapy 3 $1.7B+ $1.6B+ ~2,800 ~4,200 18 months 11 months $300M+ $374M+ ~500 ~1,000 18 months 11 months TOTAL ADDRESSABLE MARKET OPPORTUNITY Anticipate high market penetration in LGSOC KRAS mt population given: • No FDA approved therapies for LGSOC Plan to address prevalent population over 3 - 5 years from launch: • Patients cycle through therapies • Median of 3 prior therapies in RAMP 201 • Long overall survival in LGSOC patients at ~10 years • KRAS mt – ~12 years • KRAS wt – ~7 years
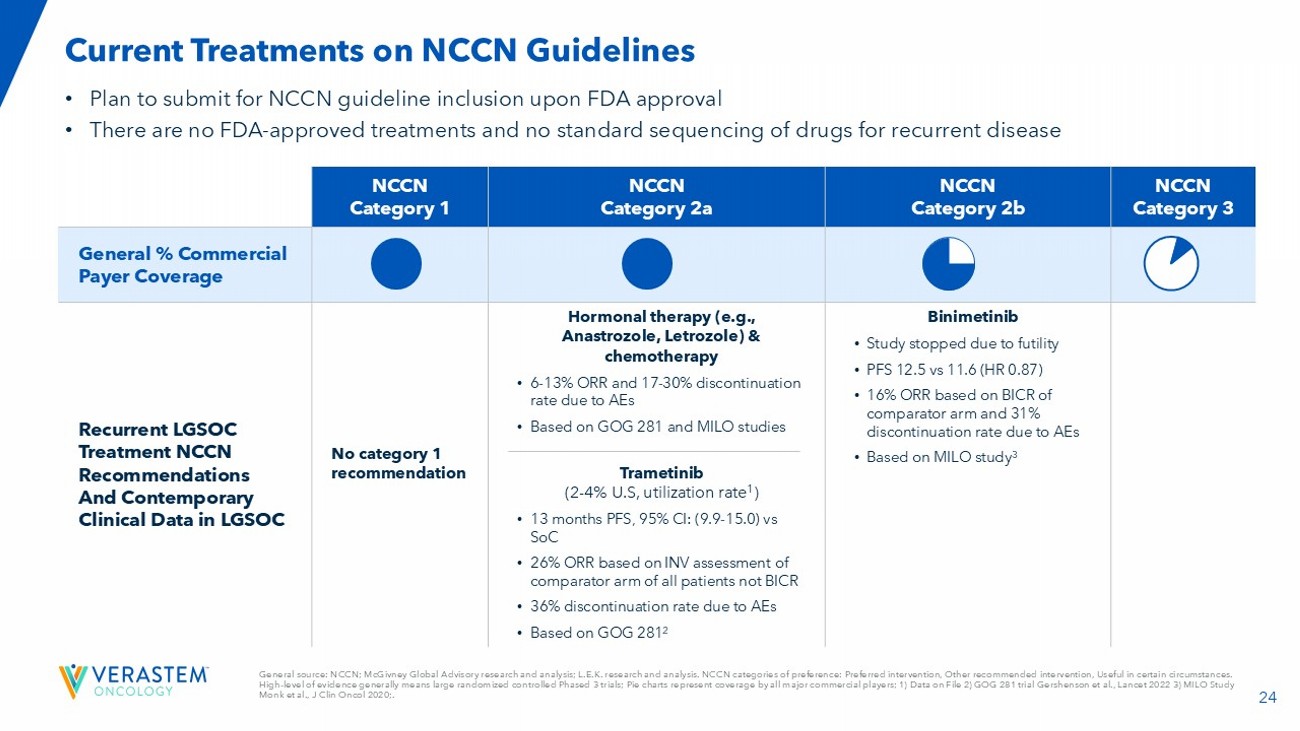
24 General source: NCCN; McGivney Global Advisory research and analysis; L.E.K. research and analysis. NCCN categories of prefer enc e: Preferred intervention, Other recommended intervention, Useful in certain circumstances. High - level of evidence generally means large randomized controlled Phased 3 trials; Pie charts represent coverage by all major c ommercial players; 1) Data on File 2) GOG 281 trial Gershenson et al., Lancet 2022 3) MILO Study Monk et al., J Clin Oncol 2020;. • Plan to submit for NCCN guideline inclusion upon FDA approval • There are no FDA - approved treatments and no standard sequencing of drugs for recurrent disease Current Treatments on NCCN Guidelines NCCN Category 3 NCCN Category 2b NCCN Category 2a NCCN Category 1 General % Commercial Payer Coverage Binimetinib • Study stopped due to futility • PFS 12.5 vs 11.6 (HR 0.87) • 16% ORR based on BICR of comparator arm and 31% discontinuation rate due to AEs • Based on MILO study 3 Hormonal therapy (e.g., Anastrozole, Letrozole) & chemotherapy • 6 - 13% ORR and 17 - 30% discontinuation rate due to AEs • Based on GOG 281 and MILO studies Trametinib (2 - 4% U.S, utilization rate 1 ) • 13 months PFS, 95% CI: (9.9 - 15.0) vs SoC • 26% ORR based on INV assessment of comparator arm of all patients not BICR • 36% discontinuation rate due to AEs • Based on GOG 281 2 No category 1 recommendation Recurrent LGSOC Treatment NCCN Recommendations And Contemporary Clinical Data in LGSOC
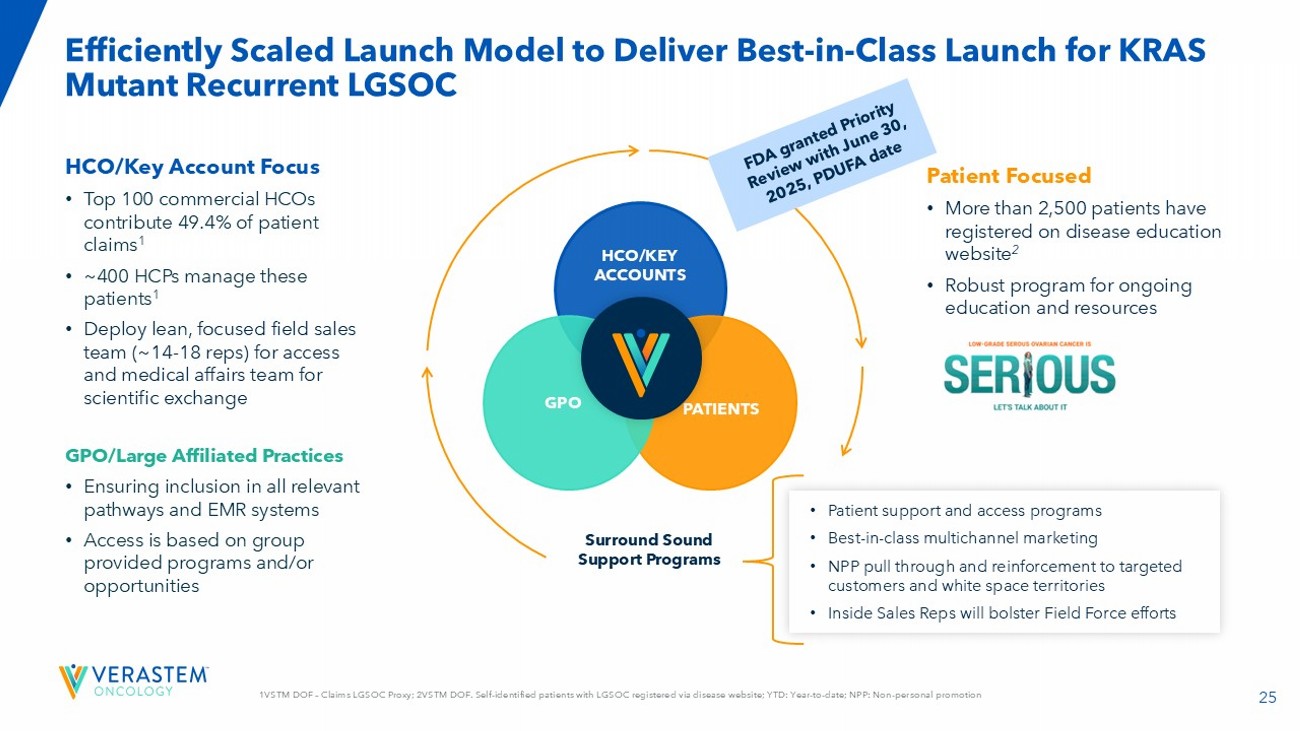
25 1VSTM DOF – Claims LGSOC Proxy; 2VSTM DOF. Self - identified patients with LGSOC registered via disease website; YTD: Year - to - date ; NPP: Non - personal promotion Efficiently Scaled Launch Model to Deliver Best - in - Class Launch for KRAS Mutant Recurrent LGSOC Surround Sound Support Programs Patient Focused • More than 2,500 patients have registered on disease education website 2 • Robust program for ongoing education and resources HCO/Key Account Focus • Top 100 commercial HCOs contribute 49.4% of patient claims 1 • ~400 HCPs manage these patients 1 • Deploy lean, focuse d field sales team (~14 - 18 reps) for access and medical affairs team for scientific exchange GPO/Large Affiliated Practices • Ensuring inclusion in all relevant pathways and EMR systems • Access is based on group provided programs and/or opportunities • Patient support and access programs • Best - in - class multichannel marketing • NPP pull through and reinforcement to targeted customers and white space territories • Inside Sales Reps will bolster Field Force efforts HCO/KEY ACCOUNTS PATIENTS GPO
26 Potential to Change Treat Paradigm and Improve Patient Outcomes 1k - 2k incidence with a prevalence of 6k - 8k; potential for high market penetration in KRAS mutant at launch enriching overtime with the prevalent patient population Current available therapies offer limited efficacy, relatively high discontinuation rates due to AEs; no FDA - approved therapies and no active promotion NCCN guidelines help to drive treatment decision ; will submit entire RAMP 201 dataset for NCCN consideration Avutometinib in combination with defactinib is differentiated on multiple efficacy measures , relatively low rates of discontinuation due to AEs and favorable tolerability Efficiently scaled launch model to deliver best - in - class launch for KRAS mutant recurrent LGSOC The combination of Avutometinib and Defactinib is an investigational drug. It has not been proven to be safe or effective and h as not been approved by FDA or any other comparable regulatory authority.
27 Next Steps in LGSOC Clinical Program and NDA Primary analysis from FRAME and RAMP 201 clinical trials anticipated to be published in H1 2025 Plan for FDA decision: June 30, 2025, PDUFA action date Plan to submit for NCCN guideline inclusion upon FDA approval Report initial data from the RAMP 201J Phase 2 clinical trial being conducted in Japan in H2 2025 Complete enrollment in RAMP 301 Phase 3 confirmatory study by end of 2025
Potential Market Expansion Opportunities in First - line Metastatic Pancreatic Cancer and Advanced Lung Cancer Avutometinib ± Defactinib
29 Topline Data from RAMP 205: Avutometinib + Defactinib + SOC in First - Line Metastatic Pancreatic Cancer
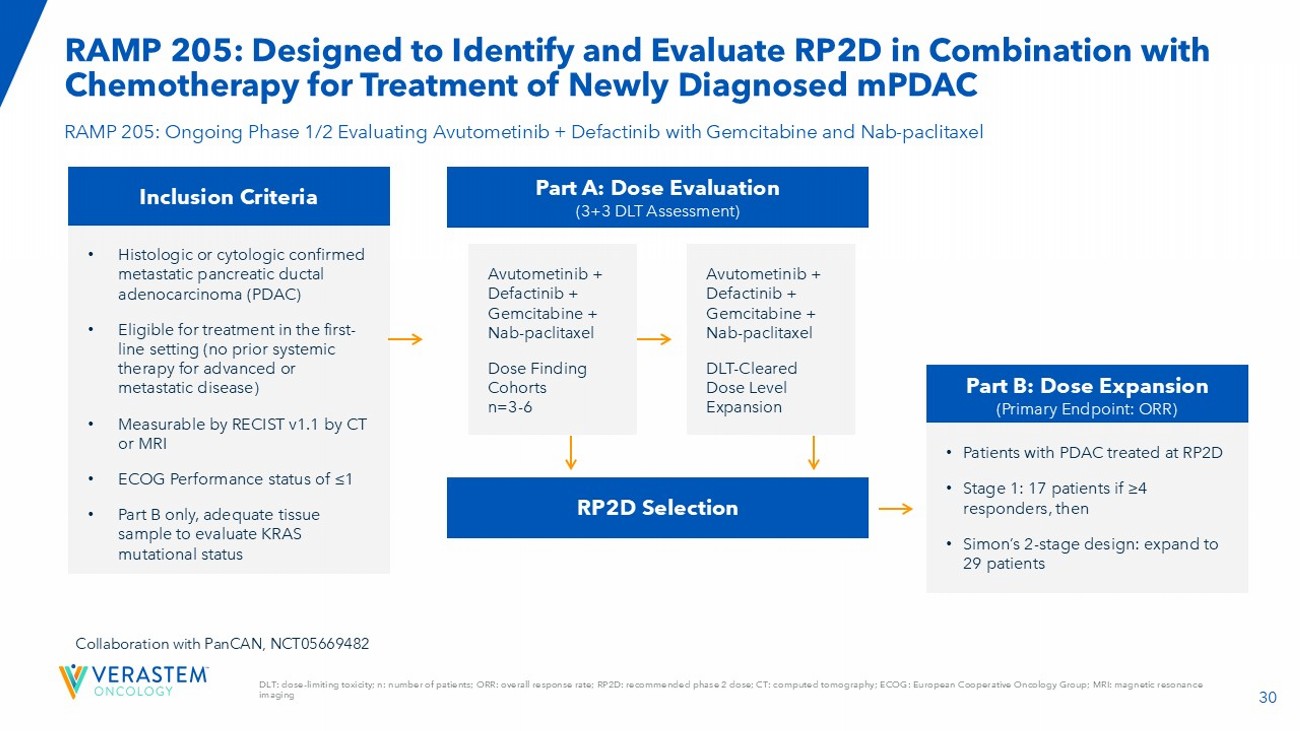
30 DLT: dose - limiting toxicity; n: number of patients; ORR: overall response rate; RP2D: recommended phase 2 dose; CT: computed tom ography; ECOG: European Cooperative Oncology Group; MRI: magnetic resonance imaging RAMP 205: Designed to Identify and Evaluate RP2D in C ombination with Chemotherapy for Tr eatment of Newly Diagnosed mPDAC RAMP 205: Ongoing Phase 1/2 Evaluating Avutometinib + Defactinib with Gemcitabine and Nab - paclitaxel Inclusion Criteria • Histologic or cytologic confirmed metastatic pancreatic ductal adenocarcinoma (PDAC) • Eligible for treatment in the first - line setting (no prior systemic therapy for advanced or metastatic disease) • Measurable by RECIST v1.1 by CT or MRI • ECOG Performance status of ≤1 • Part B only, adequate tissue sample to evaluate KRAS mutational status Collaboration with PanCAN , NCT05669482 Part A: Dose Evaluation (3+3 DLT Assessment) RP2D Selection Part B: Dose Expansion (Primary Endpoint: ORR) Avutometinib + Defactinib + Gemcitabine + Nab - paclitaxel Dose Finding Cohorts n=3 - 6 Avutometinib + Defactinib + Gemcitabine + Nab - paclitaxel DLT - Cleared Dose Level Expansion • Patients with PDAC treated at RP2D • Stage 1: 17 patients if ≥4 responders, then • Simon’s 2 - stage design: expand to 29 patients
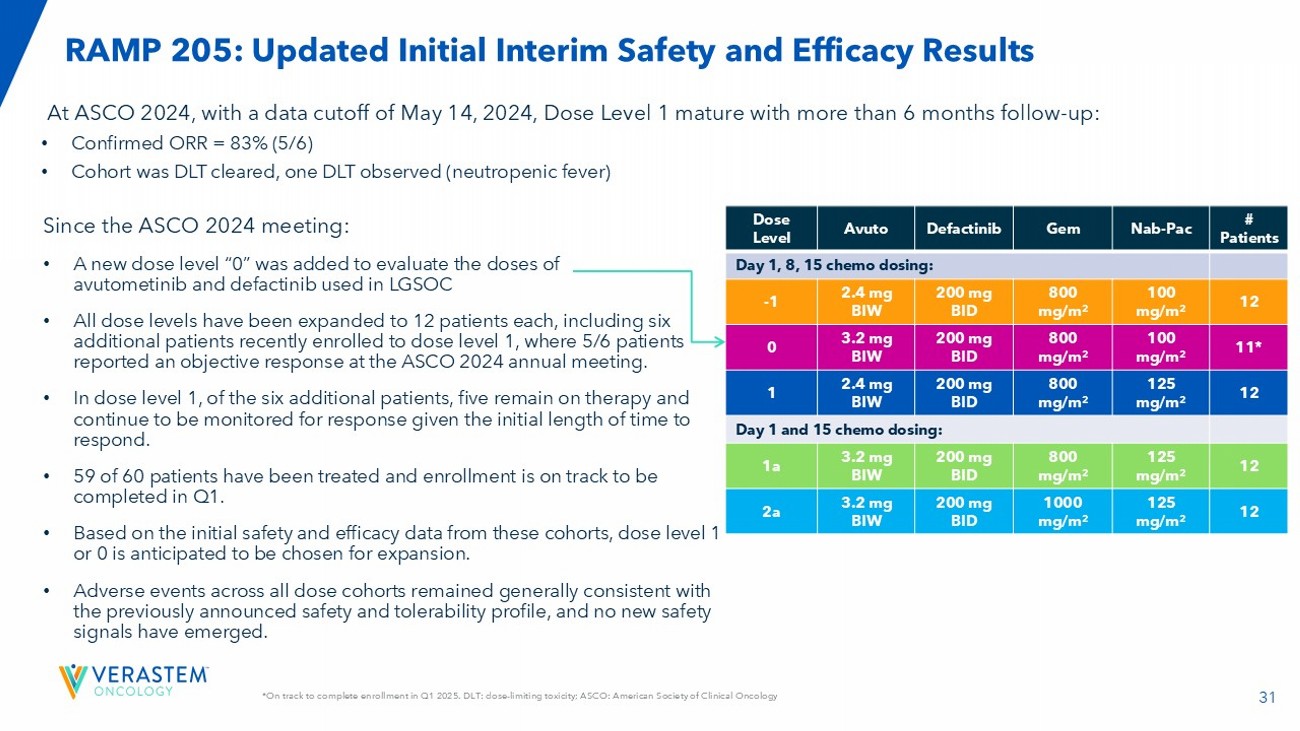
31 *On track to complete enrollment in Q1 2025. DLT: dose - limiting toxicity; ASCO: American Society of Clinical Oncology RAMP 205: Updated Initial Interim Safety and Efficacy Results # Patients Nab - Pac Gem Defactinib Avuto Dose Level Day 1, 8, 15 chemo dosing: 12 100 mg/m 2 800 mg/m 2 200 mg BID 2.4 mg BIW - 1 11* 100 mg/m 2 800 mg/m 2 200 mg BID 3.2 mg BIW 0 12 125 mg/m 2 800 mg/m 2 200 mg BID 2.4 mg BIW 1 Day 1 and 15 chemo dosing: 12 125 mg/m 2 800 mg/m 2 200 mg BID 3.2 mg BIW 1a 12 125 mg/m 2 1000 mg/m 2 200 mg BID 3.2 mg BIW 2a Since the ASCO 2024 meeting: • A new dose level “0” was added to evaluate the doses of avutometinib and defactinib used in LGSOC • All dose levels have been expanded to 12 patients each, including six additional patients recently enrolled to dose level 1, where 5/6 patients reported an objective response at the ASCO 2024 annual meeting. • In dose level 1, of the six additional patients, five remain on therapy and continue to be monitored for response given the initial length of time to respond. • 59 of 60 patients have been treated and enrollment is on track to be completed in Q1. • Based on the initial safety and efficacy data from these cohorts, dose level 1 or 0 is anticipated to be chosen for expansion. • Adverse events across all dose cohorts remained generally consistent with the previously announced safety and tolerability profile, and no new safety signals have emerged. At ASCO 2024, with a data cutoff of May 14, 2024, Dose Level 1 mature with more than 6 months follow - up: • Confirmed ORR = 83% (5/6) • Cohort was DLT cleared, one DLT observed (neutropenic fever)
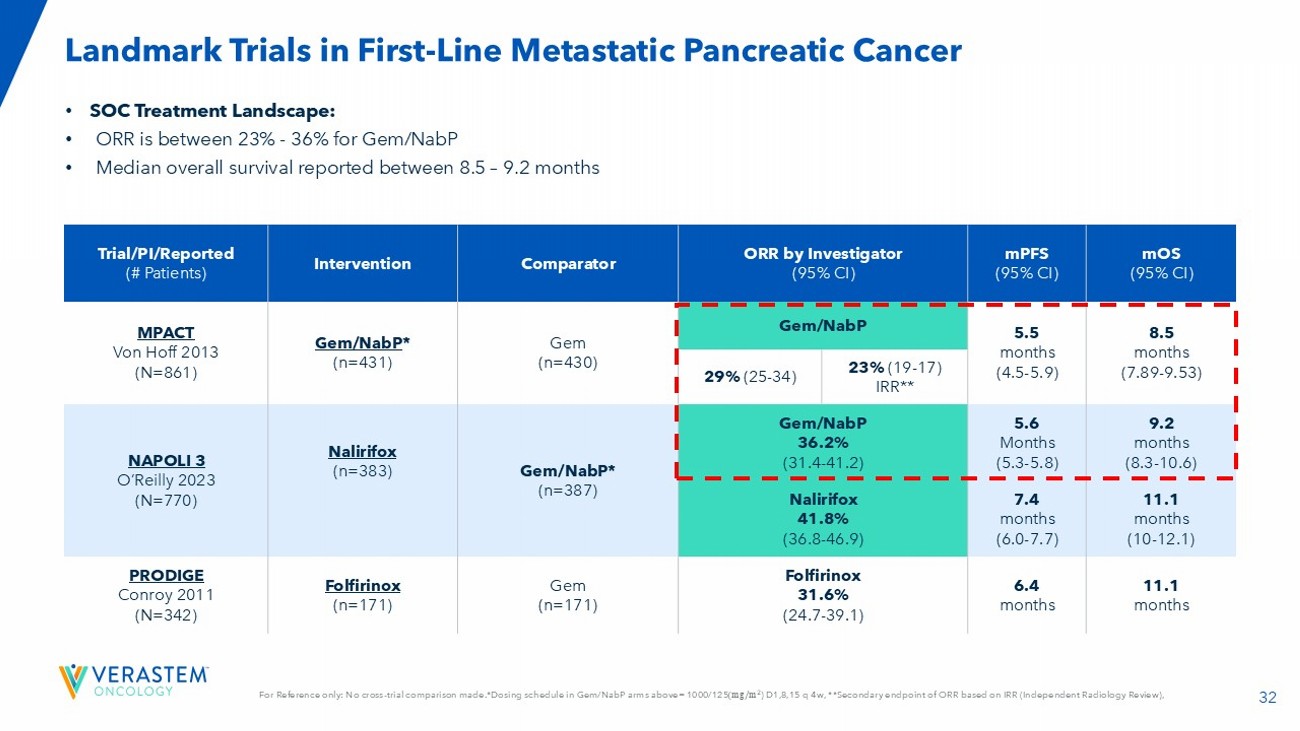
32 For Reference only: No cross - trial comparison made.*Dosing schedule in Gem/ NabP arms above= 1000/125 ሺ ‰ Ȁ ଶ ) D1,8,15 q 4w, **Secondary endpoint of ORR based on IRR (Independent Radiology Review), • SOC Treatment Landscape: • ORR is between 23% - 36% for Gem/ NabP • Median overall survival reported between 8.5 – 9.2 months Landmark Trials in First - Line Metastatic Pancreatic Cancer mOS (95% CI) mPFS (95% CI) ORR by Investigator (95% CI) Comparator Intervention Trial/PI/Reported (# Patients) 8.5 months (7.89 - 9.53) 5.5 months (4.5 - 5.9) Gem/NabP Gem (n=430) Gem/NabP * (n=431) MPACT Von Hoff 2013 (N=861) 23% (19 - 17) IRR** 29% (25 - 34) 9.2 months (8.3 - 10.6) 5.6 Months (5.3 - 5.8) Gem/NabP 36.2% (31.4 - 41.2) Gem/ NabP * (n=387) Nalirifox (n=383) NAPOLI 3 O’Reilly 2023 (N=770) 11.1 months (10 - 12.1) 7.4 months (6.0 - 7.7) Nalirifox 41.8% (36.8 - 46.9) 11.1 months 6.4 months Folfirinox 31.6% (24.7 - 39.1) Gem (n=171) Folfirinox (n=171) PRODIGE Conroy 2011 (N=342)
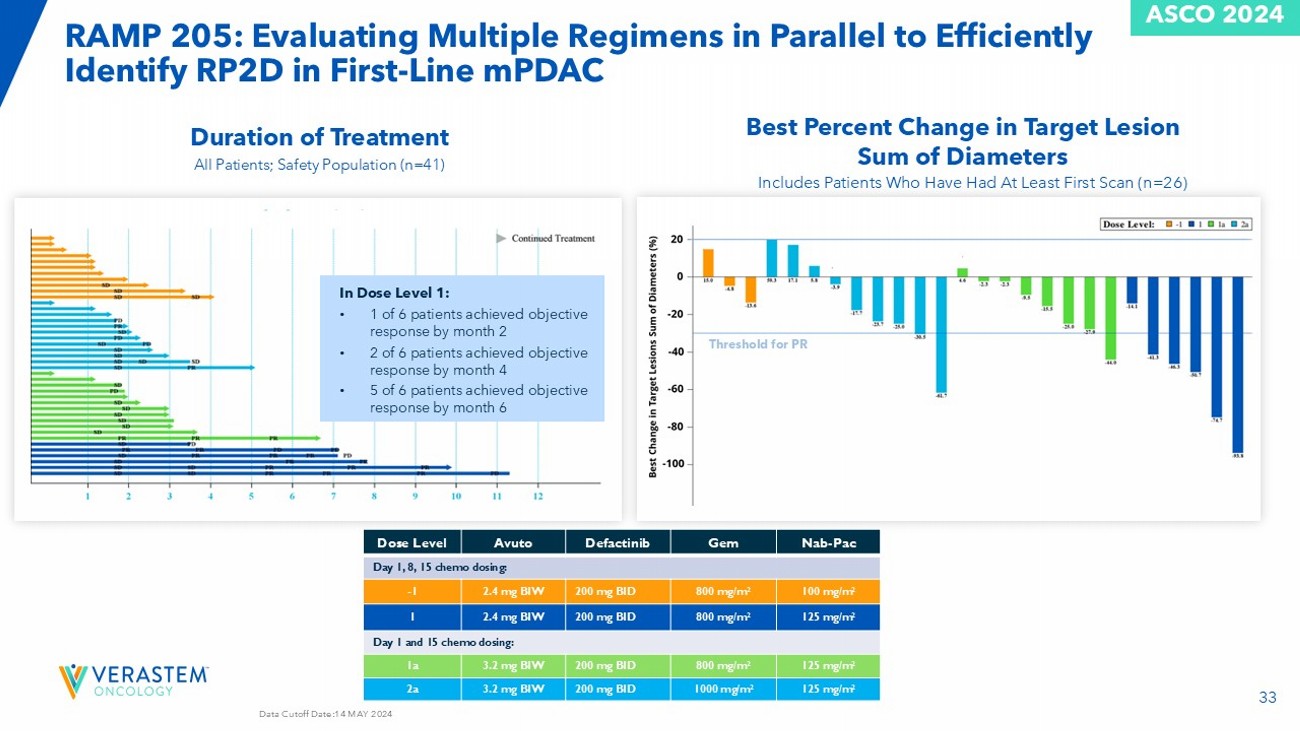
33 Data Cutoff Date:14 MAY 2024 RAMP 205: Evaluating Multiple Regimens in Parallel to Efficiently Identify RP2D in First - Line mPDAC Nab - Pac Gem Defactinib Avuto Dose Level Day 1, 8, 15 chemo dosing: 100 mg/m 2 800 mg/m 2 200 mg BID 2.4 mg BIW - 1 125 mg/m 2 800 mg/m 2 200 mg BID 2.4 mg BIW 1 Day 1 and 15 chemo dosing: 125 mg/m 2 800 mg/m 2 200 mg BID 3.2 mg BIW 1a 125 mg/m 2 1000 mg/m 2 200 mg BID 3.2 mg BIW 2a In Dose Level 1: • 1 of 6 patients achieved objective response by month 2 • 2 of 6 patients achieved objective response by month 4 • 5 of 6 patients achieved objective response by month 6 Best Percent Change in Target Lesion Sum of Diameters Includes Patients Who Have Had At Least First Scan (n=26) Threshold for PR All Patients; Safety Population (n=41) Duration of Treatment ASCO 2024
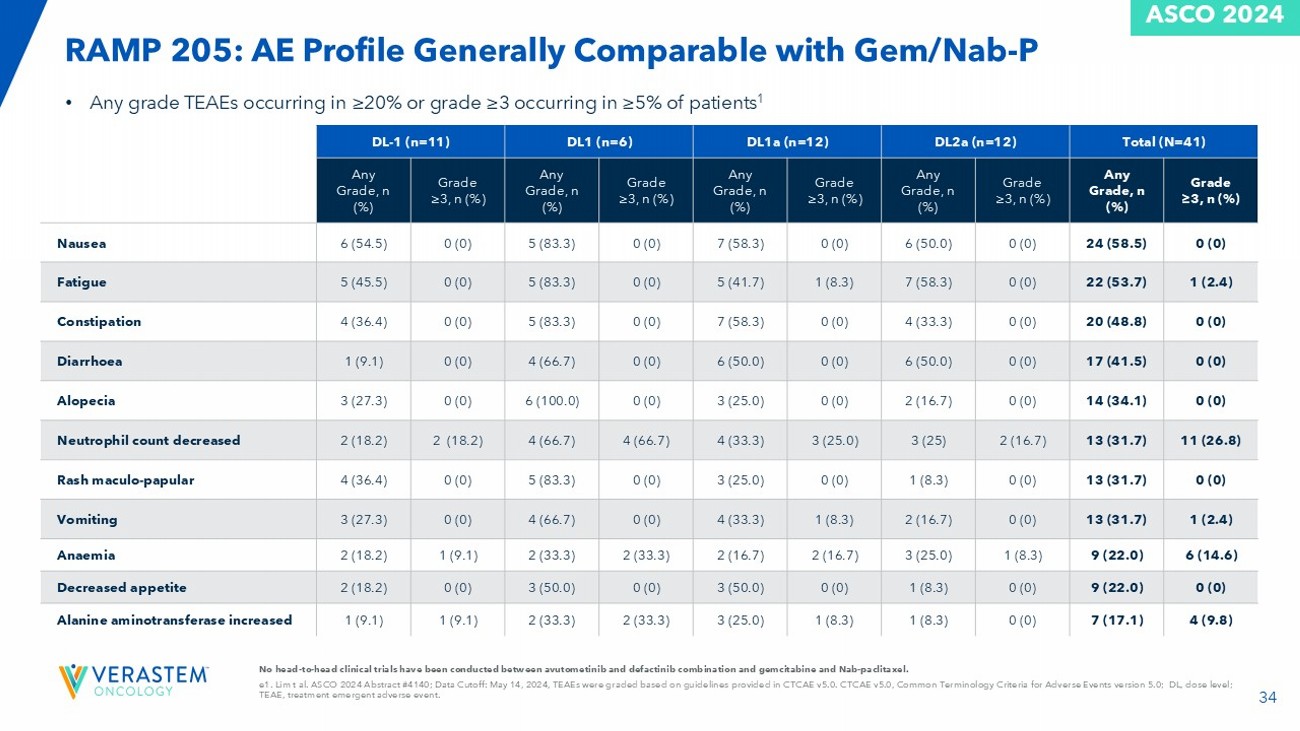
34 No head - to - head clinical trials have been conducted between avutometinib and defactinib combination and gemcitabine and Nab - pacl itaxel. e1. Lim t al. ASCO 2024 Abstract #4140; Data Cutoff: May 14, 2024, TEAEs were graded based on guidelines provided in CTCAE v5 .0. CTCAE v5.0, Common Terminology Criteria for Adverse Events version 5.0; DL, dose level; TEAE, treatment emergent adverse event. • Any grade TEAEs occurring in ≥20% or grade ≥3 occurring in ≥5% of patients 1 RAMP 205: AE Profile Generally Comparable with Gem/Nab - P Total (N=41) DL2a (n=12) DL1a (n=12) DL1 (n=6) DL - 1 (n=11) Grade ≥3, n (%) Any Grade, n (%) Grade ≥3, n (%) Any Grade, n (%) Grade ≥3, n (%) Any Grade, n (%) Grade ≥3, n (%) Any Grade, n (%) Grade ≥3, n (%) Any Grade, n (%) 0 (0) 24 (58.5) 0 (0) 6 (50.0) 0 (0) 7 (58.3) 0 (0) 5 (83.3) 0 (0) 6 (54.5) Nausea 1 (2.4) 22 (53.7) 0 (0) 7 (58.3) 1 (8.3) 5 (41.7) 0 (0) 5 (83.3) 0 (0) 5 (45.5) Fatigue 0 (0) 20 (48.8) 0 (0) 4 (33.3) 0 (0) 7 (58.3) 0 (0) 5 (83.3) 0 (0) 4 (36.4) Constipation 0 (0) 17 (41.5) 0 (0) 6 (50.0) 0 (0) 6 (50.0) 0 (0) 4 (66.7) 0 (0) 1 (9.1) Diarrhoea 0 (0) 14 (34.1) 0 (0) 2 (16.7) 0 (0) 3 (25.0) 0 (0) 6 (100.0) 0 (0) 3 (27.3) Alopecia 11 (26.8) 13 (31.7) 2 (16.7) 3 (25) 3 (25.0) 4 (33.3) 4 (66.7) 4 (66.7) 2 (18.2) 2 (18.2) Neutrophil count decreased 0 (0) 13 (31.7) 0 (0) 1 (8.3) 0 (0) 3 (25.0) 0 (0) 5 (83.3) 0 (0) 4 (36.4) Rash maculo - papular 1 (2.4) 13 (31.7) 0 (0) 2 (16.7) 1 (8.3) 4 (33.3) 0 (0) 4 (66.7) 0 (0) 3 (27.3) Vomiting 6 (14.6) 9 (22.0) 1 (8.3) 3 (25.0) 2 (16.7) 2 (16.7) 2 (33.3) 2 (33.3) 1 (9.1) 2 (18.2) Anaemia 0 (0) 9 (22.0) 0 (0) 1 (8.3) 0 (0) 3 (50.0) 0 (0) 3 (50.0) 0 (0) 2 (18.2) Decreased appetite 4 (9.8) 7 (17.1) 0 (0) 1 (8.3) 1 (8.3) 3 (25.0) 2 (33.3) 2 (33.3) 1 (9.1) 1 (9.1) Alanine aminotransferase increased ASCO 2024
35 Next Steps for RAMP 205 Plan to present additional data at a medical meeting in mid - year 2025 Select the RP2D for trial expansion in H1 2025
Avutometinib ± Defactinib with Sotorasib (G12Ci) in KRAS G12C mutant NSCLC 36
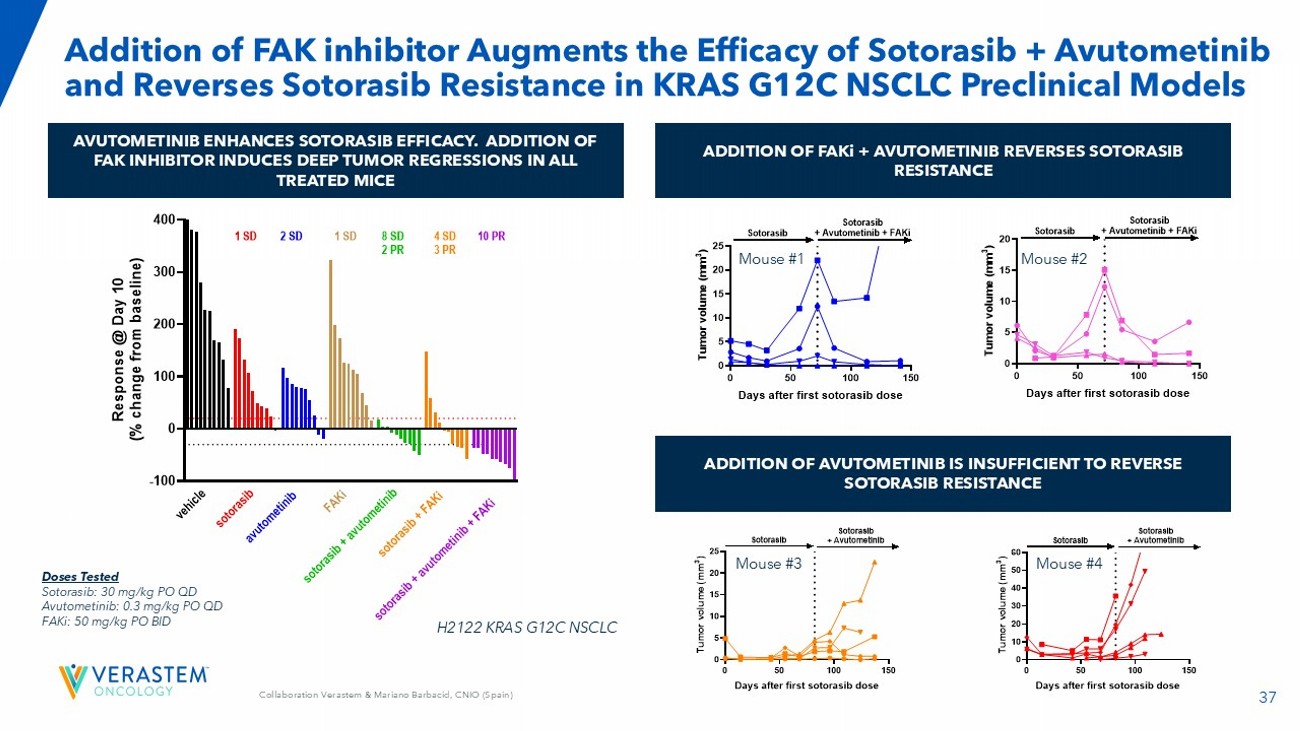
37 Collaboration Verastem & Mariano Barbacid , CNIO (Spain) Addition of FAK inhibitor Augments the Efficacy of Sotorasib + Avutometinib and Reverses Sotorasib Resistance in KRAS G12C NSCLC Preclinical Models AVUTOMETINIB ENHANCES SOTORASIB EFFICACY. ADDITION OF FAK INHIBITOR INDUCES DEEP TUMOR REGRESSIONS IN ALL TREATED MICE ADDITION OF FAKi + AVUTOMETINIB REVERSES SOTORASIB RESISTANCE ADDITION OF AVUTOMETINIB IS INSUFFICIENT TO REVERSE SOTORASIB RESISTANCE -100 0 100 200 300 400 Response at Day 10 R e s p o n s e @ D a y 1 0 ( % c h a n g e f r o m b a s e l i n e ) v e h i c l e 10 PR a v u t o m e t i n i b F A K i s o t o r a s i b s o t o r a s i b + a v u t o m e t i n i b s o t o r a s i b + F A K i s o t o r a s i b + a v u t o m e t i n i b + F A K i 2 SD 1 SD1 SD 8 SD 2 PR 4 SD 3 PR Doses Tested Sotorasib : 30 mg/kg PO QD Avutometinib : 0.3 mg/kg PO QD FAKi : 50 mg/kg PO BID H2122 KRAS G12C NSCLC 0 50 100 150 0 5 10 15 20 25 Days after first sotorasib dose T u m o r v o l u m e ( m m 3 ) Sotorasib + Avutometinib + FAKiSotorasib 0 50 100 150 0 5 10 15 20 25 Days after first sotorasib dose T u m o r v o l u m e ( m m 3 ) Sotorasib + Avutometinib Sotorasib Mouse #1 Mouse #2 Mouse #3 Mouse #4
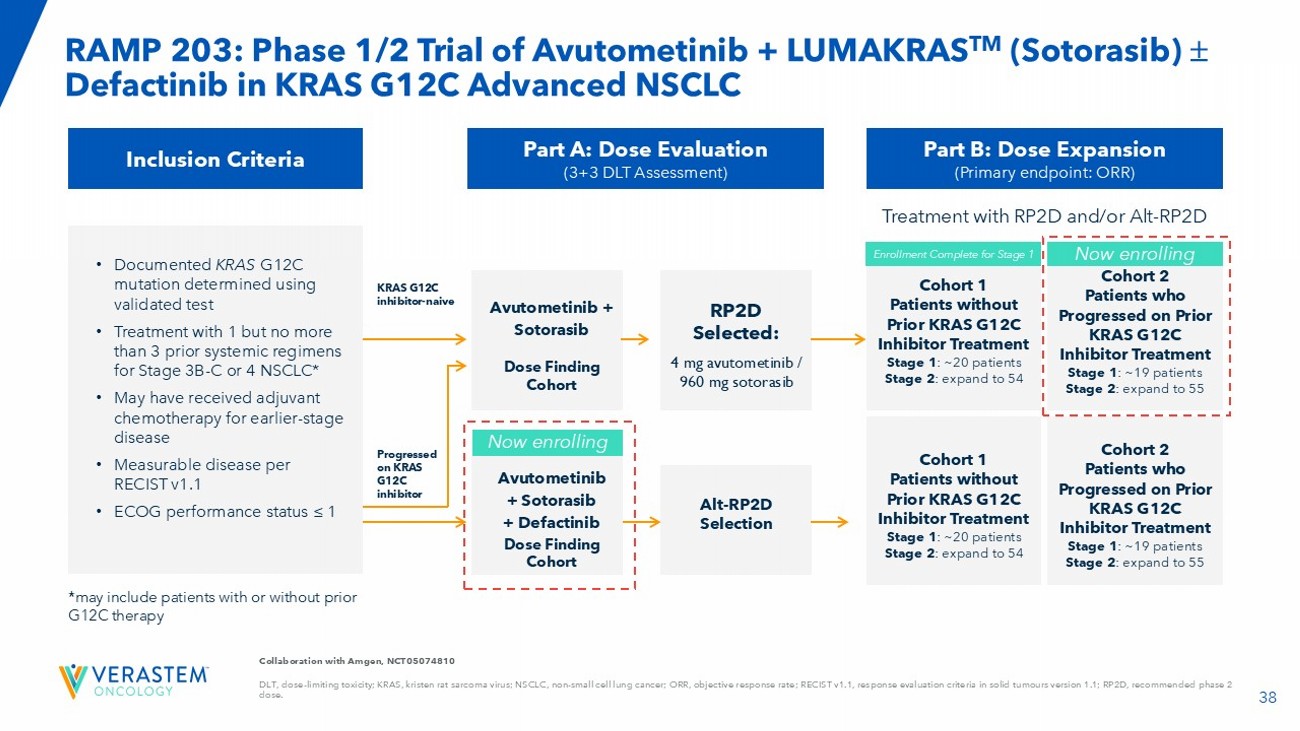
38 Collaboration with Amgen, NCT05074810 DLT, dose - limiting toxicity; KRAS, kristen rat sarcoma virus; NSCLC, non - small cell lung cancer; ORR, objective response rate; RECIST v1.1, response evaluation criteria i n solid tumours version 1.1; RP2D, recommended phase 2 dose. RAMP 203: Phase 1/2 Trial of Avutometinib + LUMAKRAS TM ( Sotorasib ) Defactinib in KRAS G12C Advanced NSCLC Inclusion Criteria • Documented KRAS G12C mutation determined using validated test • Treatment with 1 but no more than 3 prior systemic regimens for Stage 3B - C or 4 NSCLC* • May have received adjuvant chemotherapy for earlier - stage disease • Measurable disease per RECIST v1.1 • ECOG performance status ≤ 1 Part A: Dose Evaluation (3+3 DLT Assessment) Avutometinib + Sotorasib Dose Finding Cohort Part B: Dose Expansion (Primary endpoint: ORR) RP2D Selected: 4 mg a vutometinib / 960 mg sotorasib Avutometinib + Sotorasib + Defactinib Dose Finding Cohort Alt - RP2D Selection KRAS G12C inhibitor - naive Progressed on KRAS G12C inhibitor Now enrolling Cohort 1 Patients without Prior KRAS G12C Inhibitor Treatment Stage 1 : ~20 patients Stage 2 : expand to 54 Cohort 2 Patients who Progressed on Prior KRAS G12C Inhibitor Treatment Stage 1 : ~19 patients Stage 2 : expand to 55 Cohort 1 Patients without Prior KRAS G12C Inhibitor Treatment Stage 1 : ~20 patients Stage 2 : expand to 54 Cohort 2 Patients who Progressed on Prior KRAS G12C Inhibitor Treatment Stage 1 : ~19 patients Stage 2 : expand to 55 Enrollment Complete for Stage 1 Now enrolling *may include patients with or without prior G12C therapy Treatment with RP2D and/or Alt - RP2D
39 RAMP 203: No DLTs Were Observed in the First Triplet Combination Cohort in Patients Previously Treated with a G12C Inhibitor Triplet Combination Update: • As of a November 21, 2024 , data cutoff, 3 patients whose cancer previously progressed on a G12C inhibitor have been treated with the triplet combination of sotorasib 960 mg administered daily on a continuous schedule and avutometinib 3.2 mg twice - weekly (BIW) plus defactinib 200 mg twice - daily (BID). Avutometinib and defactinib are administered on a three out of four weeks schedule. • 2 of the 3 patients demonstrated initial tumor reductions of at least 20% at the first scan. As of the data cutoff, all three patients remain on treatment. • With no DLTs observed in the first triplet combination cohort, enrollment of additional patients to the triplet combination continues. Doublet Combination Update: • As previously reported, the doublet combination of avutometinib with sotorasib has completed enrollment (n=28) in the G12C inhibitor treatment - naïve Stage 1 Part B cohort. • Enrollment to the KRAS G 12 C inhibitor, prior - treated Stage 1 Part B doublet cohort on track to complete in Q 1 2025 . • Patients enrolled in the doublet cohorts continue to be followed for safety and efficacy results (both the prior - treated and treatment - naïve cohorts) . • Plan to complete enrollment and evaluate the safety and efficacy of the triplet combination before expanding either of the doublet cohorts .
40 Next Steps for RAMP 203 Plan to present an interim update of both doublet and triplet data at a medical meeting in H2 2025
Partnership with GenFleet Therapeutics on Novel, Potential Best - in - Class RAS Pathway - Related Programs 41
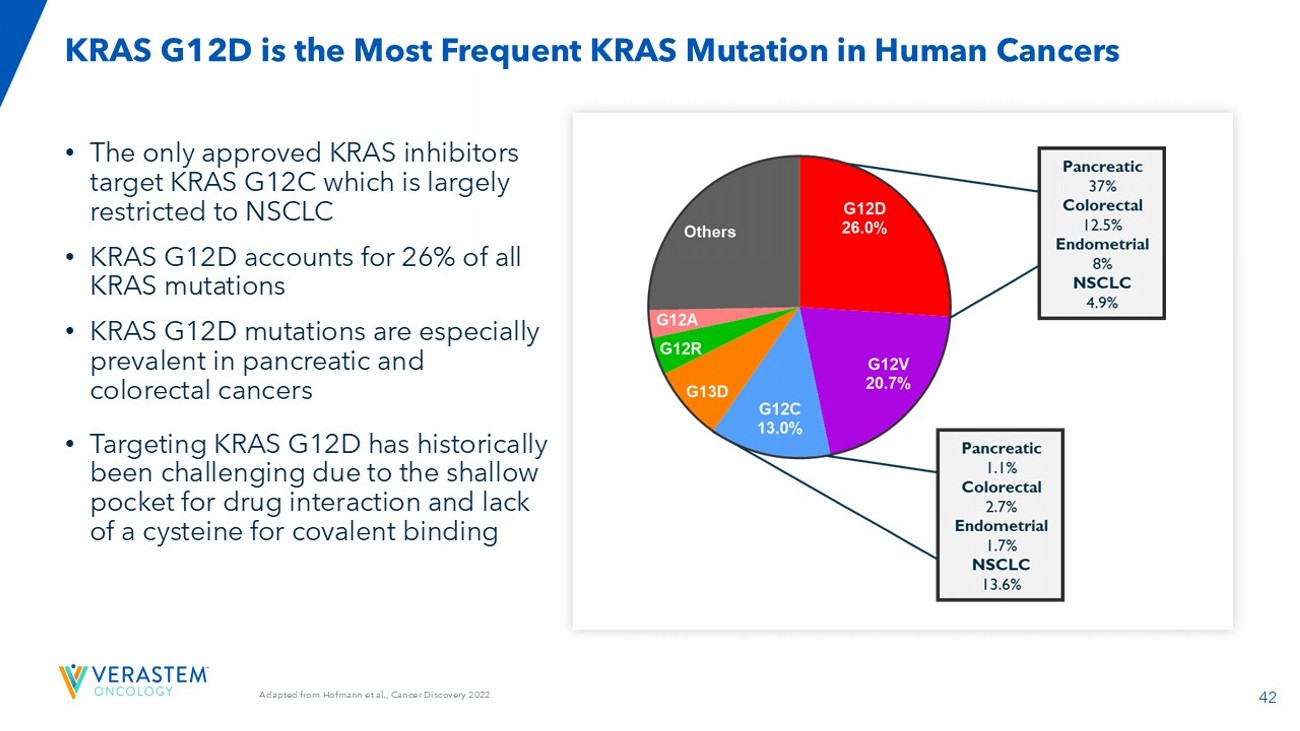
42 Adapted from Hofmann et al., Cancer Discovery 2022 • The only approved KRAS inhibitors target KRAS G12C which is largely restricted to NSCLC • KRAS G12D accounts for 26% of all KRAS mutations • KRAS G12D mutations are especially prevalent in pancreatic and colorectal cancers • Targeting KRAS G12D has historically been challenging due to the shallow pocket for drug interaction and lack of a cysteine for covalent binding KRAS G12D is the Most Frequent KRAS Mutation in Human Cancers
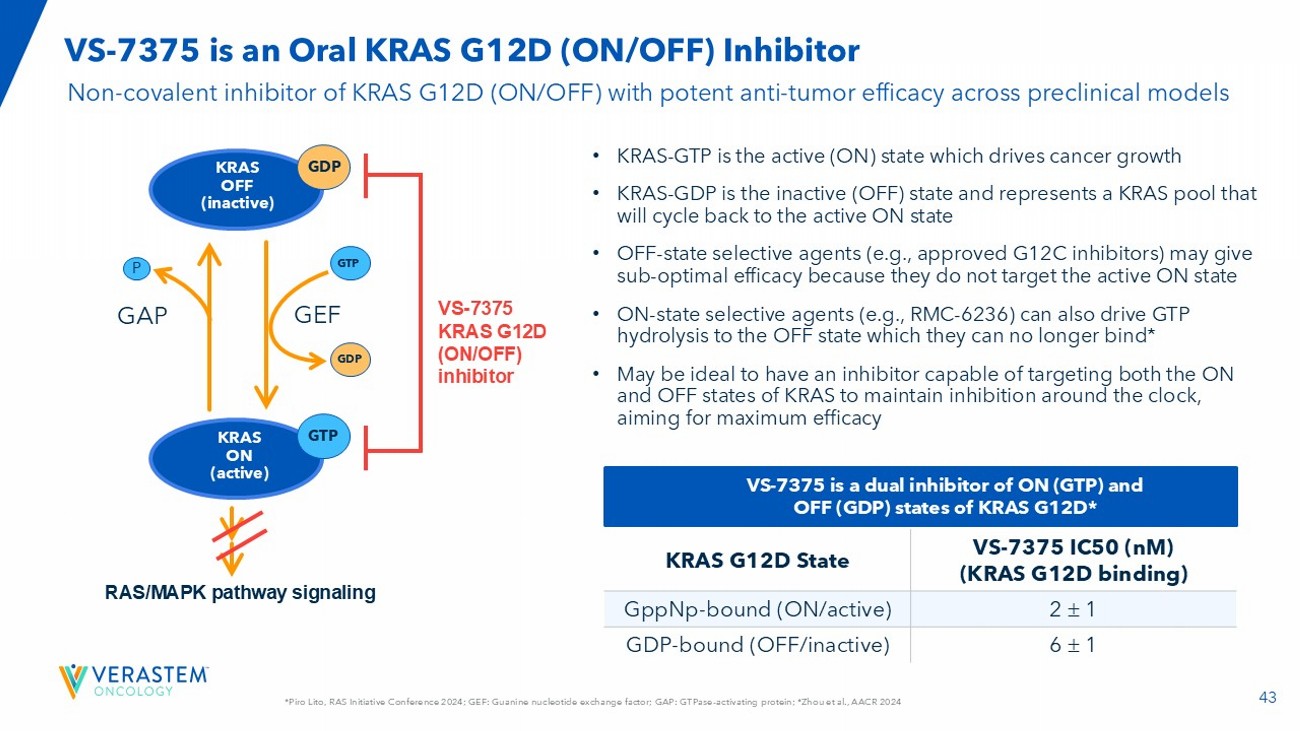
43 *Piro Lito, RAS Initiative Conference 2024; GEF: Guanine nucleotide exchange factor; GAP: GTPase - activating protein; *Zhou et al ., AACR 2024 VS - 7375 is an Oral KRAS G12D (ON/OFF) Inhibitor GEF GTP GDP GTP GDP RAS/MAPK pathway signaling GAP P KRAS OFF (inactive) KRAS ON (active) VS - 7375 KRAS G12D (ON/OFF) inhibitor VS - 7375 IC50 ( nM ) (KRAS G12D binding) KRAS G12D State 2 1 GppNp - bound (ON/active) 6 1 GDP - bound (OFF/inactive) VS - 7375 is a dual inhibitor of ON (GTP) and OFF (GDP) states of KRAS G12D* Non - covalent inhibitor of KRAS G12D (ON/OFF) with potent anti - tumor efficacy across preclinical models • KRAS - GTP is the active (ON) state which drives cancer growth • KRAS - GDP is the inactive (OFF) state and represents a KRAS pool that will cycle back to the active ON state • OFF - state selective agents (e.g., approved G12C inhibitors) may give sub - optimal efficacy because they do not target the active ON state • ON - state selective agents (e.g., RMC - 6236) can also drive GTP hydrolysis to the OFF state which they can no longer bind* • May be ideal to have an inhibitor capable of targeting both the ON and OFF states of KRAS to maintain inhibition around the clock, aiming for maximum efficacy
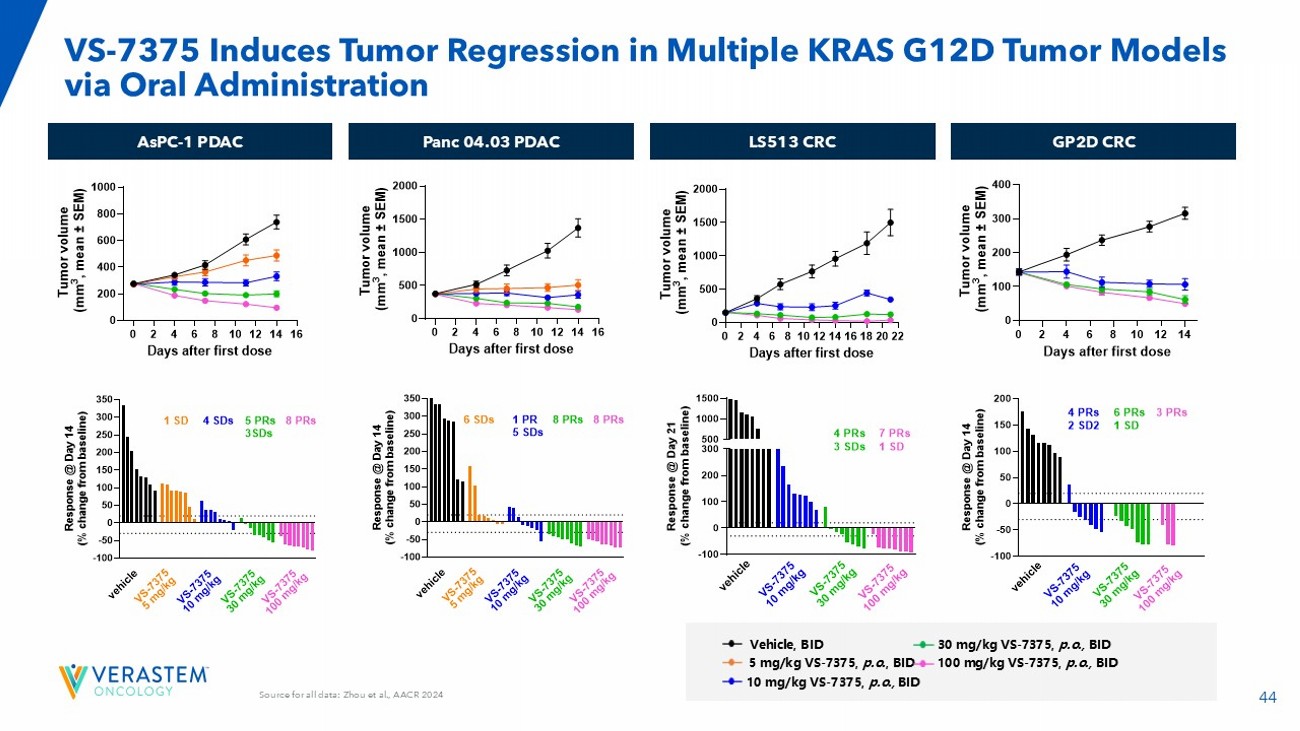
44 Source for all data: Zhou et al., AACR 2024 VS - 7375 Induces Tumor Regression in Multiple KRAS G12D Tumor Models via Oral Administration AsPC - 1 PDAC Panc 04.03 PDAC LS513 CRC GP2D CRC 0 2 4 6 8 10 12 14 16 0 200 400 600 800 1000 Days after first dose T u m o r v o l u m e ( m m 3 , m e a n ± S E M ) 0 2 4 6 8 10 12 14 16 0 500 1000 1500 2000 Days after first dose T u m o r v o l u m e ( m m 3 , m e a n ± S E M ) 0 2 4 6 8 10121416182022 0 500 1000 1500 2000 Days after first dose T u m o r v o l u m e ( m m 3 , m e a n ± S E M ) 5 mg/kg VS - 7 375, p .o. , BID Vehicle, BID 10 mg/kg VS - 7 375, p .o., BID 30 mg/kg VS - 7 375, p .o., BID 100 mg/kg VS - 7 375, p .o., BID -100 -50 0 50 100 150 200 250 300 350 R e s p o n s e @ D a y 1 4 ( % c h a n g e f r o m b a s e l i n e ) v e h i c l e V S - 7 3 7 5 1 0 m g / k g V S - 7 3 7 5 3 0 m g / k g V S - 7 3 7 5 1 0 0 m g / k g 6 SDs 1 PR 5 SDs 8 PRs 8 PRs V S - 7 3 7 5 5 m g / k g -100 -50 0 50 100 150 200 250 300 350 R e s p o n s e @ D a y 1 4 ( % c h a n g e f r o m b a s e l i n e ) v e h i c l e V S - 7 3 7 5 1 0 m g / k g V S - 7 3 7 5 3 0 m g / k g V S - 7 3 7 5 1 0 0 m g / k g V S - 7 3 7 5 5 m g / k g 1 SD 4 SDs 5 PRs 3SDs 8 PRs -100 0 100 200 300 500 1000 1500 R e s p o n s e @ D a y 2 1 ( % c h a n g e f r o m b a s e l i n e ) v e h i c l e V S - 7 3 7 5 1 0 m g / k g V S - 7 3 7 5 3 0 m g / k g V S - 7 3 7 5 1 0 0 m g / k g 4 PRs 3 SDs 7 PRs 1 SD
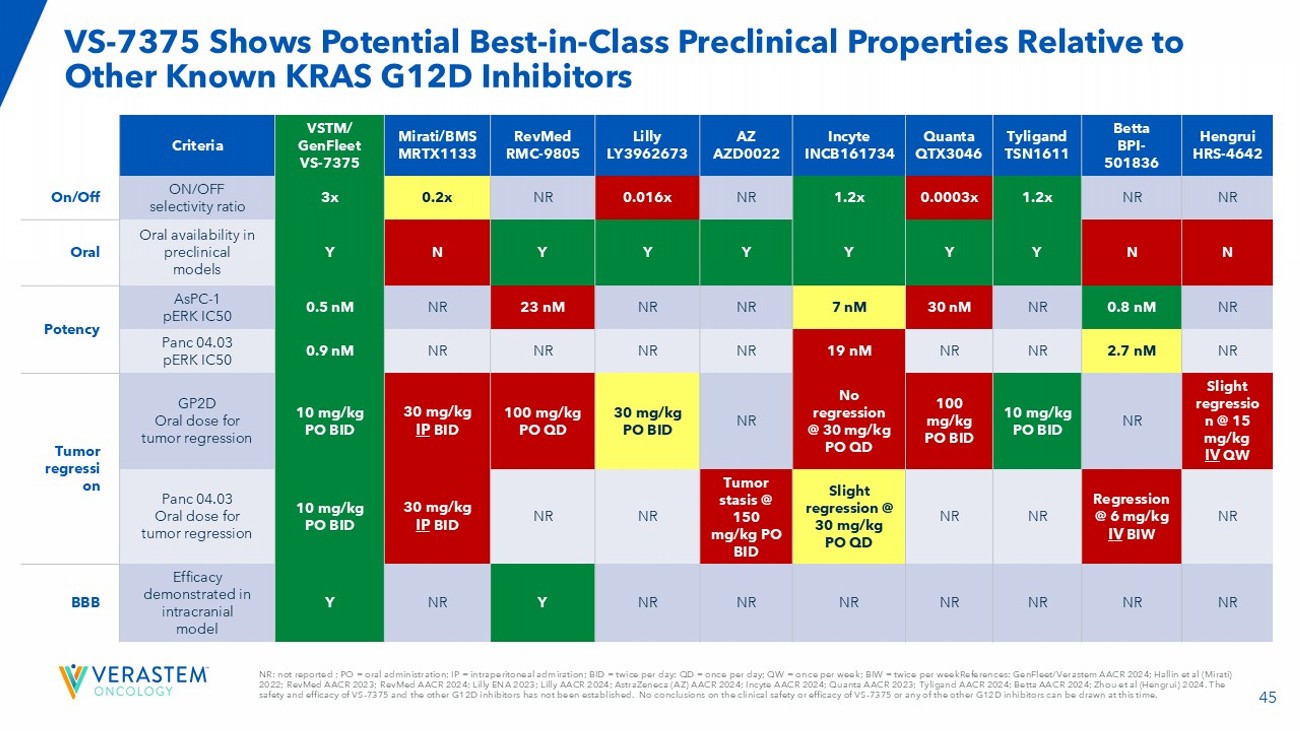
45 NR: not reported ; PO = oral administration; IP = intraperitoneal admiration; BID = twice per day; QD = once per day; QW = on ce per week; BIW = twice per weekReferences : GenFleet / Verastem AACR 2024; Hallin et al (Mirati) 2022; RevMed AACR 2023; RevMed AACR 2024; Lilly ENA 2023; Lilly AACR 2024; AstraZeneca (AZ) AACR 2024; Incyte AACR 2024; Quanta AACR 2023; Tyligand AACR 2024; Betta AACR 2024; Zhou et al ( Hengrui ) 2024. The safety and efficacy of VS - 7375 and the other G12D inhibitors has not been established. No conclusions on the clinical safety or efficacy of VS - 7375 or any of the other G12D inhibitors can be drawn at this time. VS - 7375 Shows Potential Best - in - Class Preclinical Properties Relative to Other Known KRAS G12D Inhibitors Hengrui HRS - 4642 Betta BPI - 501836 Tyligand TSN1611 Quanta QTX3046 Incyte INCB161734 AZ AZD0022 Lilly LY3962673 RevMed RMC - 9805 Mirati/BMS MRTX1133 VSTM/ GenFleet VS - 7375 Criteria NR NR 1.2x 0.0003x 1.2x NR 0.016x NR 0.2x 3x ON/OFF selectivity ratio On/Off N N Y Y Y Y Y Y N Y Oral availability in preclinical models Oral NR 0.8 nM NR 30 nM 7 nM NR NR 23 nM NR 0.5 nM AsPC - 1 pERK IC50 Potency NR 2.7 nM NR NR 19 nM NR NR NR NR 0.9 nM Panc 04.03 pERK IC50 Slight regressio n @ 15 mg/kg IV QW NR 10 mg/kg PO BID 100 mg/kg PO BID No regression @ 30 mg/kg PO QD NR 30 mg/kg PO BID 100 mg/kg PO QD 30 mg/kg IP BID 10 mg/kg PO BID GP2D Oral dose for tumor regression Tumor regressi on NR Regression @ 6 mg/kg IV BIW NR NR Slight regression @ 30 mg/kg PO QD Tumor stasis @ 150 mg/kg PO BID NR NR 30 mg/kg IP BID 10 mg/kg PO BID Panc 04.03 Oral dose for tumor regression NR NR NR NR NR NR NR Y NR Y Efficacy demonstrated in intracranial model BBB
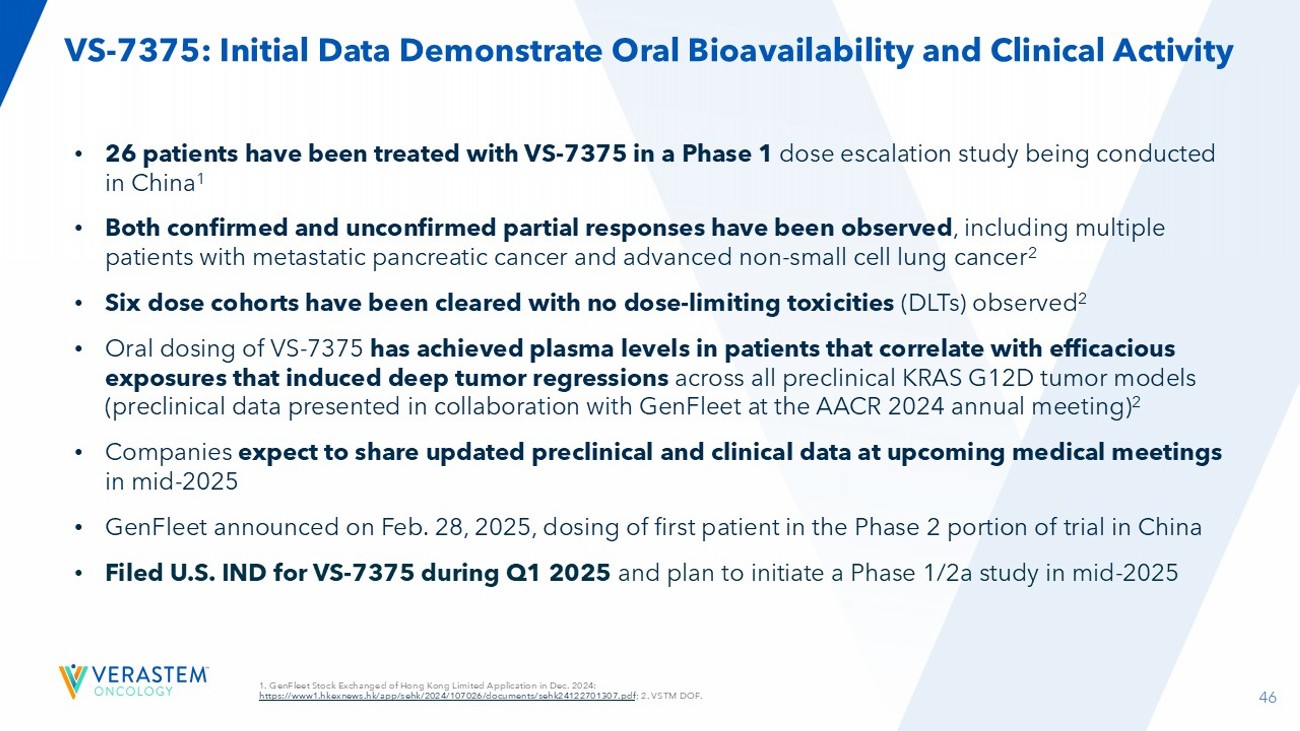
46 VS - 7375: Initial Data Demonstrate Oral Bioavailability and Clinical Activity • 26 patients have been treated with VS - 7375 in a Phase 1 dose escalation study being conducted in China 1 • Both confirmed and unconfirmed partial responses have been observed , including multiple patients with metastatic pancreatic cancer and advanced non - small cell lung cancer 2 • Six dose cohorts have been cleared with no dose - limiting toxicities (DLTs) observed 2 • Oral dosing of VS - 7375 has achieved plasma levels in patients that correlate with efficacious exposures that induced deep tumor regressions across all preclinical KRAS G12D tumor models (preclinical data presented in collaboration with GenFleet at the AACR 2024 annual meeting ) 2 • Companies expect to share updated preclinical and clinical data at upcoming medical meetings in mid - 2025 • GenFleet announced on Feb. 28, 2025, dosing of first patient in the Phase 2 portion of trial in China • Filed U.S. IND for VS - 7375 during Q1 2025 and plan to initiate a Phase 1/2a study in mid - 2025 1. GenFleet Stock Exchanged of Hong Kong Limited Application in Dec. 2024: https://www1.hkexnews.hk/app/sehk/2024/107026/documents/sehk24122701307.pdf ; 2. VSTM DOF.
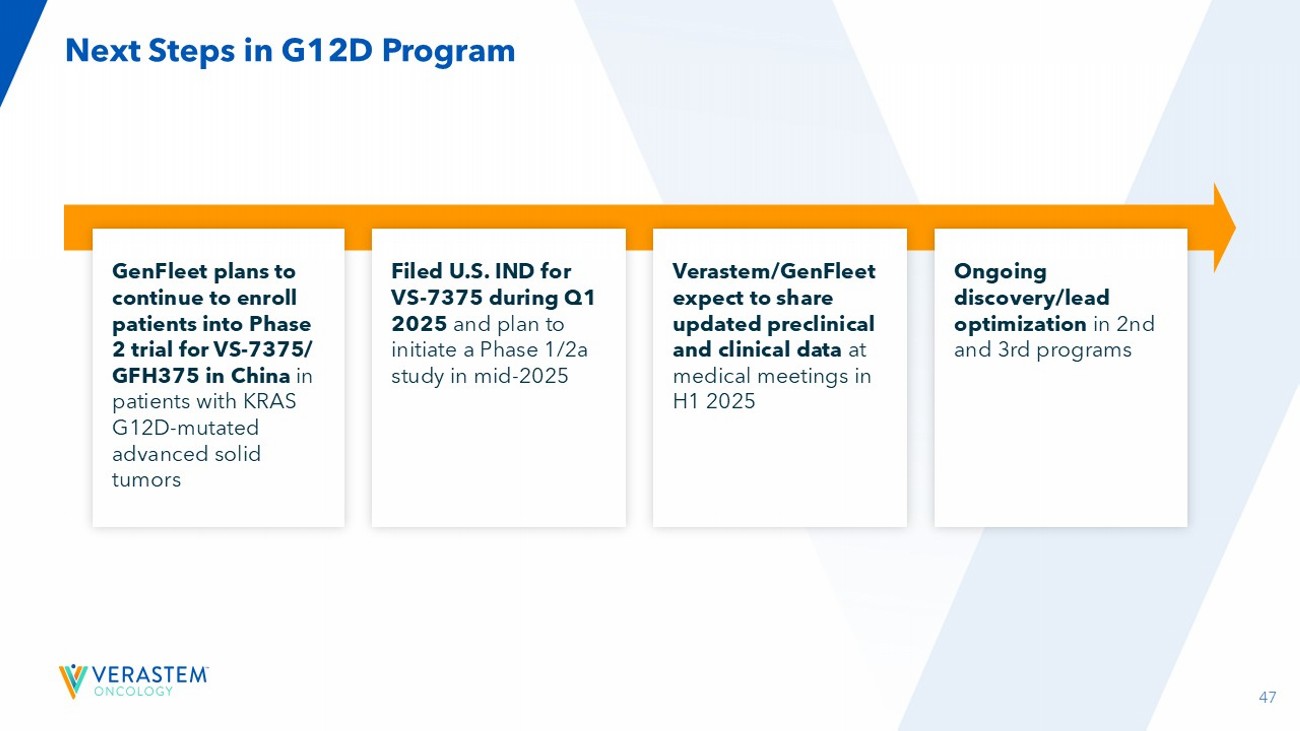
47 Next Steps in G12D Program GenFleet plans to continue to enroll patients into Phase 2 trial for VS - 7375/ GFH375 in China in patients with KRAS G12D - mutated advanced solid tumors Verastem/GenFleet expect to share updated preclinical and clinical data at medical meetings in H1 2025 Filed U.S. IND for VS - 7375 during Q1 2025 and plan to initiate a Phase 1/2a study in mid - 2025 Ongoing discovery/lead optimization in 2nd and 3rd programs

48 Anticipated Milestones & Financials 48
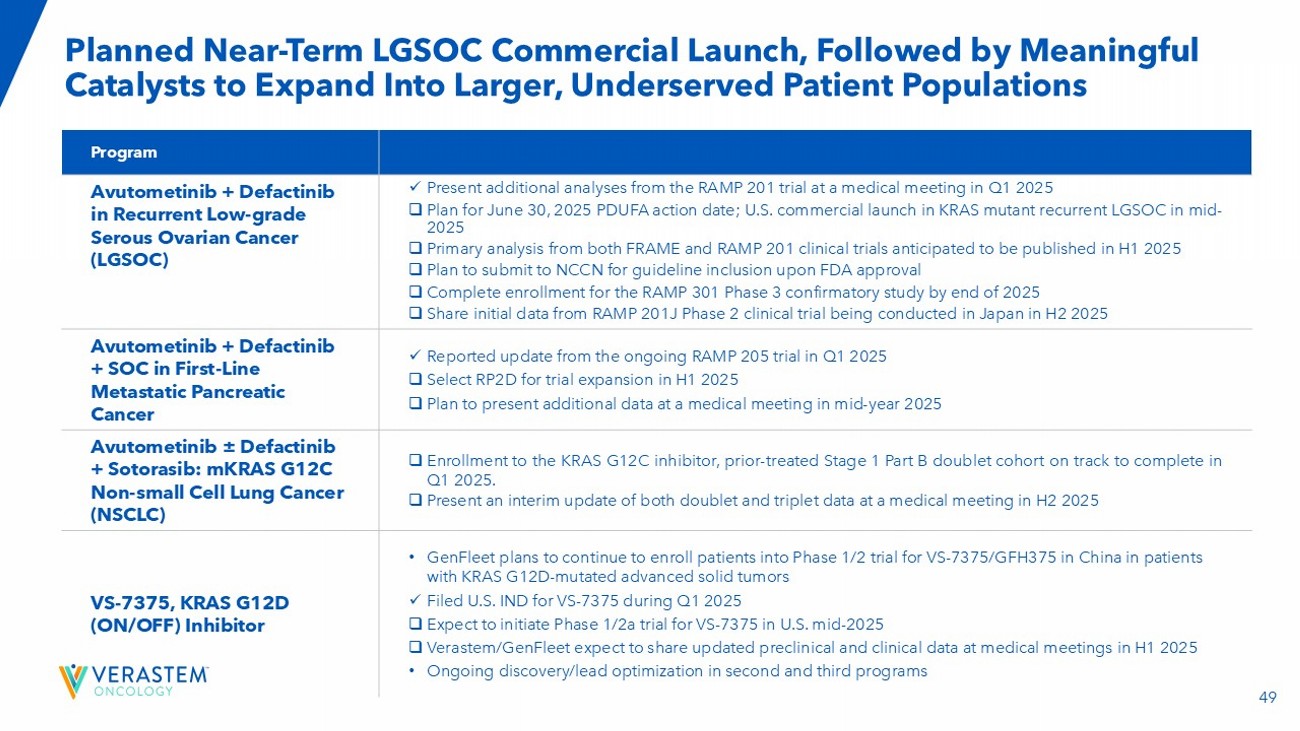
49 Planned Near - Term LGSOC Commercial Launch, Followed by Meaningful Catalysts to Expand Into Larger, Underserved Patient Populations Anticipated Milestones & Activities Program x Present additional analyses from the RAMP 201 trial at a medical meeting in Q1 2025 □ Plan for June 30, 2025 PDUFA action date ; U.S. commercial launch in KRAS mutant recurrent LGSOC in mid - 2025 □ Primary analysis from both FRAME and RAMP 201 clinical trials anticipated to be published in H1 2025 □ Plan to submit to NCCN for guideline inclusion upon FDA approval □ Complete enrollment for the RAMP 301 Phase 3 confirmatory study by end of 2025 □ Share initial data from RAMP 201J Phase 2 clinical trial being conducted in Japan in H2 2025 Avutometinib + Defactinib in Recurrent Low - grade Serous Ovarian Cancer (LGSOC) x Reported update from the ongoing RAMP 205 trial in Q1 2025 □ Select RP2D for trial expansion in H1 2025 □ Plan to present additional data at a medical meeting in mid - year 2025 Avutometinib + Defactinib + SOC in First - Line Metastatic Pancreatic Cancer □ Enrollment to the KRAS G 12 C inhibitor, prior - treated Stage 1 Part B doublet cohort on track to complete in Q 1 2025 . □ Present an interim update of both doublet and triplet data at a medical meeting in H2 2025 Avutometinib ± Defactinib + Sotorasib: mKRAS G12C Non - small Cell Lung Cancer (NSCLC) • GenFleet plans to continue to enroll patients into Phase 1/2 trial for VS - 7375/GFH375 in China in patients with KRAS G12D - mutated advanced solid tumors x Filed U.S. IND for VS - 7375 during Q1 2025 □ Expect to initiate Phase 1/2a trial for VS - 7375 in U.S. mid - 2025 □ Verastem/GenFleet expect to share updated preclinical and clinical data at medical meetings in H1 2025 • Ongoing discovery/lead optimization in second and third programs VS - 7375, KRAS G12D (ON/OFF) Inhibitor
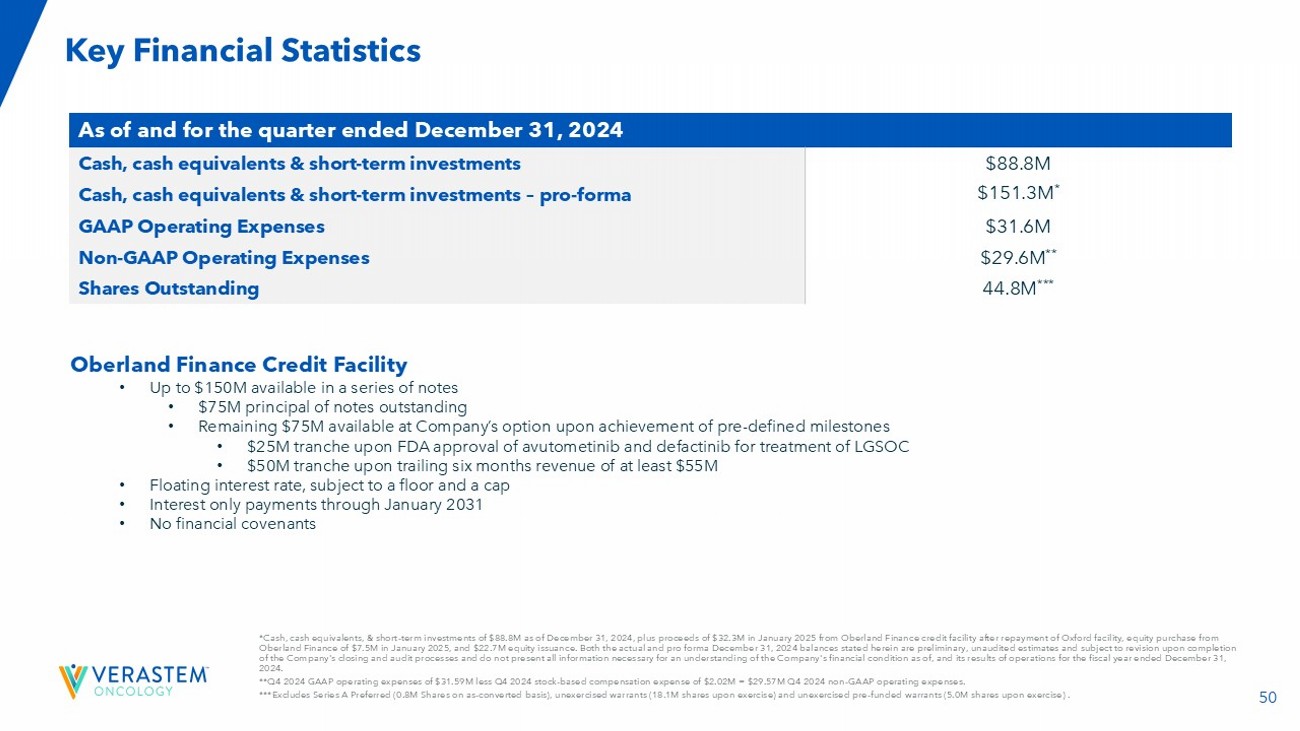
50 *Cash, cash equivalents, & short - term investments of $88.8M as of December 31, 2024, plus proceeds of $32.3M in January 2025 fro m Oberland Finance credit facility after repayment of Oxford facility, equity purchase from Oberland Finance of $7.5M in January 2025, and $22.7M equity issuance. Both the actual and pro forma December 31, 2024 balanc es stated herein are preliminary, unaudited estimates and subject to revision upon completion of the Company's closing and audit processes and do not present all information necessary for an understanding of the Company 's financial condition as of, and its results of operations for the fiscal year ended December 31, 2024. **Q4 2024 GAAP operating expenses of $31.59M less Q4 2024 stock - based compensation expense of $2.02M = $29.57M Q4 2024 non - GAAP operating expenses. ***Excludes Series A Preferred (0.8M Shares on as - converted basis), unexercised warrants (18.1M shares upon exercise) and unexer cised pre - funded warrants (5.0M shares upon exercise) . Key Financial Statistics As of and for the quarter ended December 31, 2024 $88.8M Cash, cash equivalents & short - term investments $151.3M * Cash, cash equivalents & short - term investments – pro - forma $31.6M GAAP Operating Expenses $29.6M ** Non - GAAP Operating Expenses 44.8M *** Shares Outstanding Oberland Finance Credit Facility • Up to $150M available in a series of notes • $75M principal of notes outstanding • Remaining $75M available at Company’s option upon achievement of pre - defined milestones • $25M tranche upon FDA approval of avutometinib and defactinib for treatment of LGSOC • $50M tranche upon trailing six months revenue of at least $55M • Floating interest rate, subject to a floor and a cap • Interest only payments through January 2031 • No financial covenants

THANK YOU! 51

Addendum
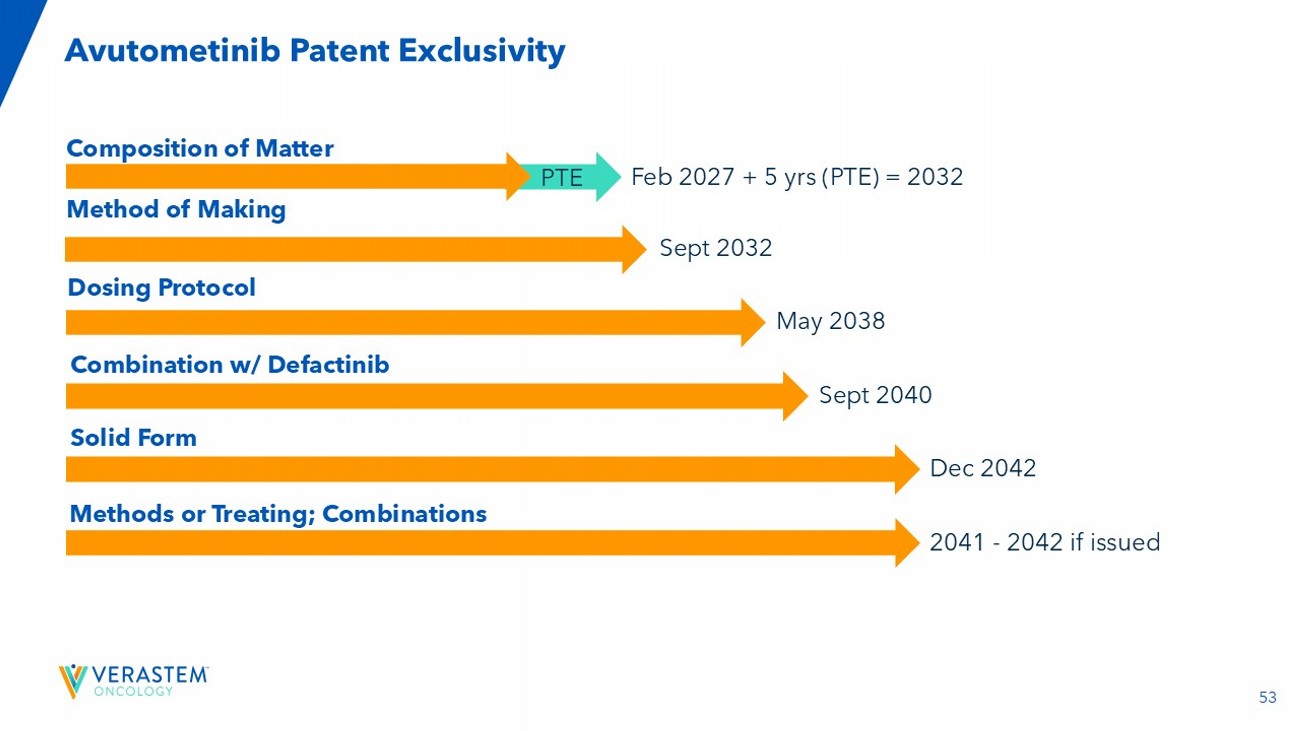
53 Avutometinib Patent Exclusivity Composition of Matter Method of Making Sept 2032 Dosing Protocol May 2038 Combination w/ Defactinib Dec 2042 Feb 2027 + 5 yrs (PTE) = 2032 Sept 2040 Solid Form PTE 2041 - 2042 if issued Methods or Treating; Combinations

54 Experienced Senior Management Team Cathy Carew Chief Organizationa l Effectiveness Officer Colleen Mockbee Global Head of Regulatory Affairs and Development Nate Sanburn Chief Business Officer Dan Calkins Chief Financial Officer Matt Ros Chief Operating Officer Mike Crowther Chief Commercial & Strategy Officer Jonathan Pachter, Ph.D. Chief Scientific Officer John Hayslip, M.D. Chief Medical Officer Daniel Paterson President and CEO • Principal – HR Collaborative • Ironwood, ActiveBiotics , Dynogen , Tufts Health Plan • Chief Developmen t Officer & SVP of Regulatory, OncXerna • Head of Global Regulatory, Lilly Oncology • Associate VP, Head of Collaborations & Late Phase BD, Lilly Oncology • National Gene Vector Lab, Indiana Univer sity • Technical Accounting Consultant - CFGI • PwC LLP • CEO, FORE Biotherapeut ics • EVP & CSBO, Epizyme • COO, Sanofi - Genzyme • BMS • CBO, Minerva Biotechnolo gies • Interim US lead and VP of US Marketing, Kite Pharma • Celgene • Head of Cancer Biology – OSI (now Astellas) • Schering - Plough • CMO, I - MAB • Nektar Therapeutics , AbbVie • University of Kentucky’s Markey Cancer Center • CEO, The DNA Repair Co. (now On - Q - ity ) • PharMetrics (now IMS) • Axion Previous experience
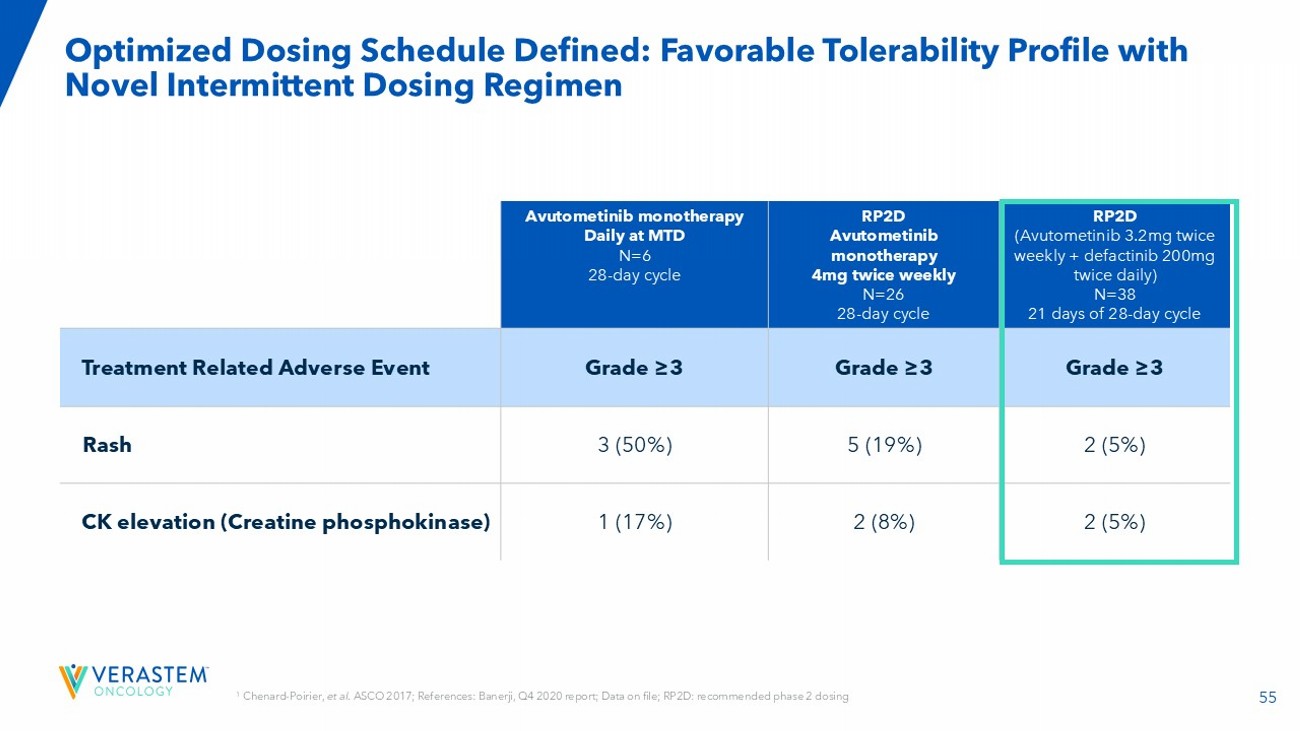
55 Optimized Dosing Schedule Defined: Favorable Tolerability Profile with Novel Intermittent Dosing Regimen RP2D (Avutometinib 3.2mg twice weekly + defactinib 200mg twice daily) N=38 21 days of 28 - day cycle RP2D Avutometinib monotherapy 4mg twice weekly N=26 28 - day cycle Avutometinib monotherapy Daily at MTD N=6 28 - day cycle Grade ≥3 Grade ≥3 Grade ≥3 Treatment Related Adverse Event 2 (5%) 5 (19%) 3 (50%) Rash 2 (5%) 2 (8%) 1 (17%) CK elevation (Creatine phosphokinase) 1 Chenard - Poirier, et al . ASCO 2017; References: Banerji, Q4 2020 report; Data on file; RP2D: recommended phase 2 dosing
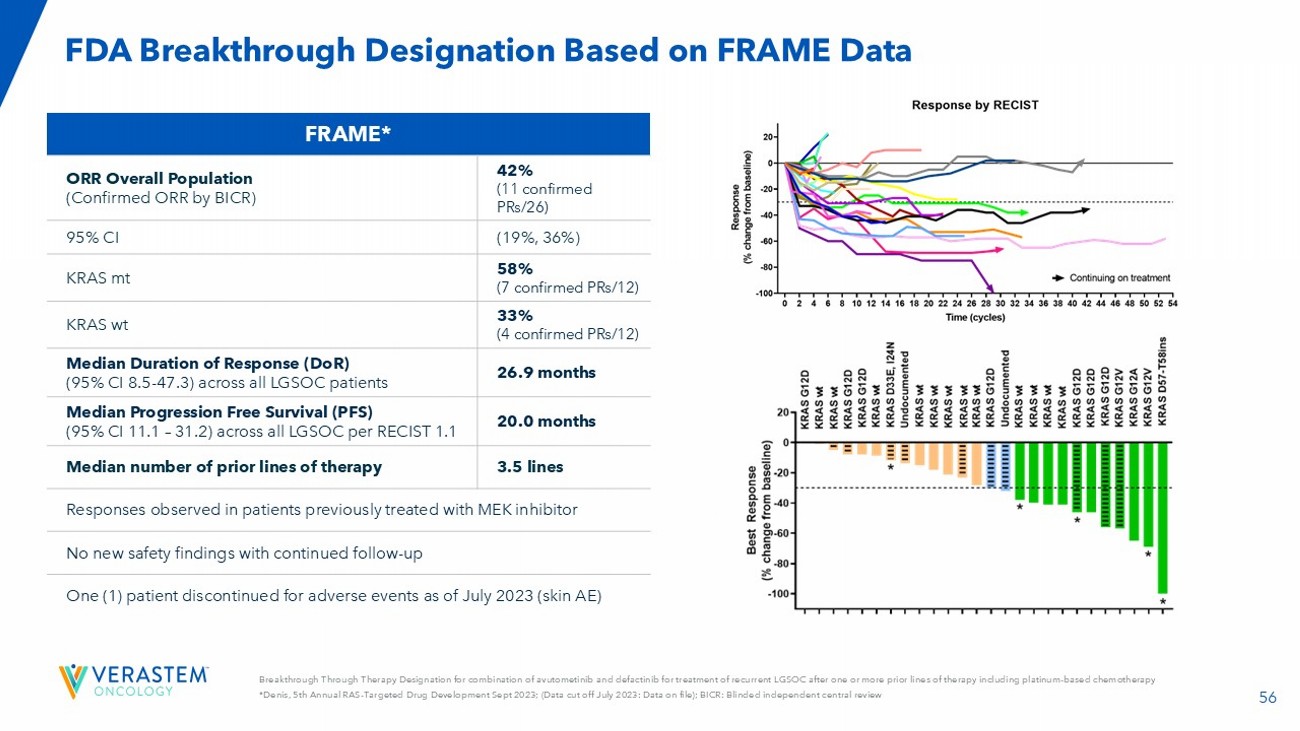
56 Breakthrough Through Therapy Designation for combination of avutometinib and defactinib for treatment of recurrent LGSOC after one or more prior lines of therapy including platinum - based chemotherapy *Denis, 5th Annual RAS - Targeted Drug Development Sept 2023; (Data cut off July 2023: Data on file); BICR: Blinded independent central review FDA Breakthrough Designation Based on FRAME Data FRAME* 42% (11 confirmed PRs/26) ORR Overall Population (Confirmed ORR by BICR) (19%, 36%) 95% CI 58% (7 confirmed PRs/12) KRAS mt 33% (4 confirmed PRs/12) KRAS wt 26.9 months Median Duration of Response ( DoR ) (95% CI 8.5 - 47.3) across all LGSOC patients 20.0 months Median Progression Free Survival (PFS) (95% CI 11.1 – 31.2) across all LGSOC per RECIST 1.1 3.5 lines Median number of prior lines of therapy Responses observed in patients previously treated with MEK inhibitor No new safety findings with continued follow - up One (1) patient discontinued for adverse events as of July 2023 (skin AE)
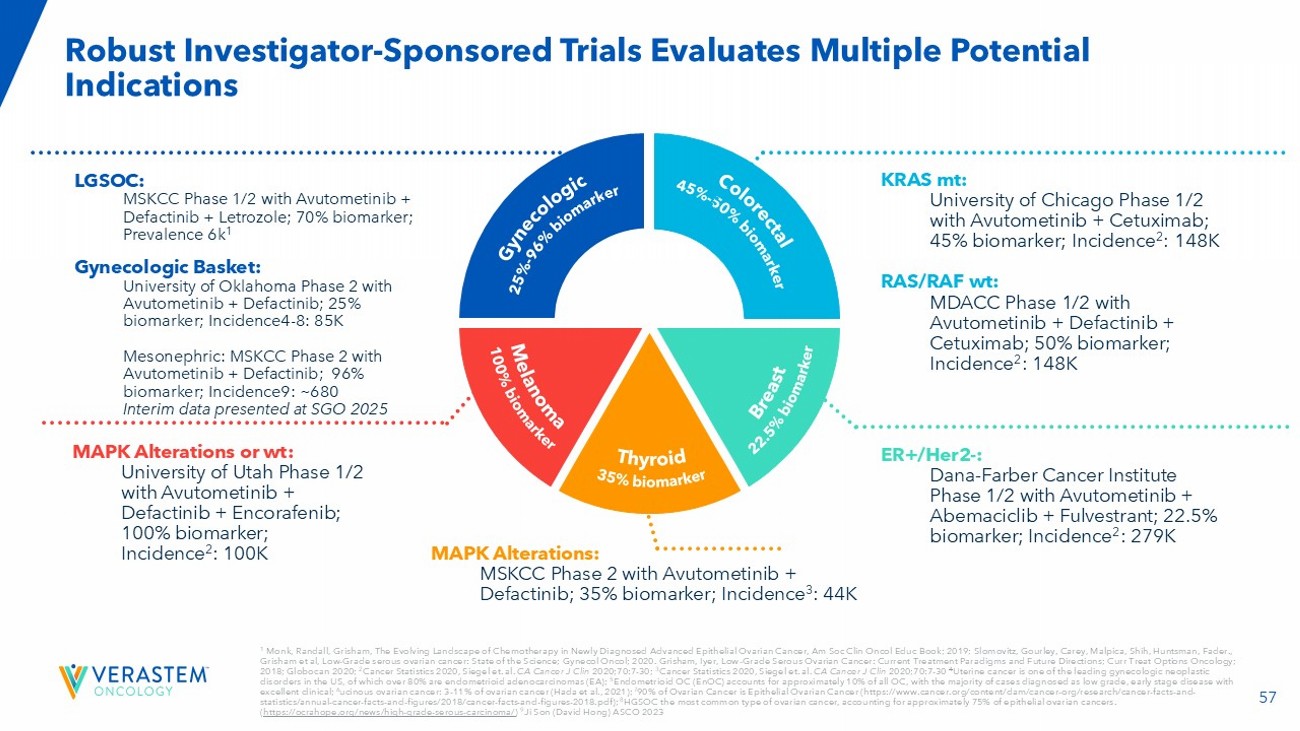
57 1 Monk, Randall, Grisham, The Evolving Landscape of Chemotherapy in Newly Diagnosed Advanced Epithelial Ovarian Cancer, Am Soc Cl in Oncol Educ Book; 2019; Slomovitz , Gourley, Carey, Malpica, Shih, Huntsman, Fader., Grisham et al, Low - Grade serous ovarian cancer: State of the Science; Gynecol Oncol; 2020. Grisham, Iyer, Low - Grade Serous Ovarian Cancer: Current Treatment Paradigms and Future Directions; Curr Treat Opti ons Oncology; 2018; Globocan 2020; 2 Cancer Statistics 2020, Siegel et. al. CA Cancer J Clin 2020;70:7 - 30 ; 3 Cancer Statistics 2020, Siegel et. al. CA Cancer J Clin 2020;70:7 - 30 4 Uterine cancer is one of the leading gynecologic neoplastic disorders in the US, of which over 80% are endometrioid adenocarcinomas (EA); 5 Endometrioid OC ( EnOC ) accounts for approximately 10% of all OC, with the majority of cases diagnosed as low grade, early stage disease with excellent clinical; 6 ucinous ovarian cancer: 3 - 11% of ovarian cancer (Hada et al., 2021); 7 90% of Ovarian Cancer is Epithelial Ovarian Cancer (https:// www.cancer.org /content/dam/cancer - org/research/cancer - facts - and - statistics/annual - cancer - facts - and - figures/2018/cancer - facts - and - figures - 2018.pdf); 8 HGSOC the most common type of ovarian cancer, accounting for approximately 75% of epithelial ovarian cancers. ( https://ocrahope.org/news/high - grade - serous - carcinoma/ ) 9 Ji Son (David Hong) ASCO 2023 Robust Investigator - Sponsored Trials Evaluates Multiple Potential Indications LGSOC: MSKCC Phase 1/2 with Avutometinib + Defactinib + Letrozole; 70% biomarker; Prevalence 6k 1 Gynecologic Basket: University of Oklahoma Phase 2 with Avutometinib + Defactinib ; 25% biomarker; Incidence4 - 8: 85K Mesonephric: MSKCC Phase 2 with Avutometinib + Defactinib; 96% biomarker; Incidence9: ~680 Interim data presented at SGO 2025 KRAS mt: University of Chicago Phase 1/2 with Avutometinib + Cetuximab; 45% biomarker; Incidence 2 : 148K RAS/RAF wt : MDACC Phase 1/2 with Avutometinib + Defactinib + Cetuximab; 50% biomarker; Incidence 2 : 148K ER+/Her2 - : Dana - Farber Cance r Institute Phase 1/2 with Avutometinib + Abemaciclib + Fulvestrant ; 22.5% biomarker; Incidence 2 : 279K MAPK Alterations or wt : University of Utah Phase 1/2 with Avutometinib + Defactinib + Encorafenib ; 100% biomarker; Incidence 2 : 100K MAPK Alterations: MSKCC Phase 2 with Avutometinib + Defactinib ; 35% biomarker; Incidence 3 : 44K
v3.25.1
Cover
|
Mar. 20, 2025 |
| Cover [Abstract] |
|
| Document Type |
8-K
|
| Amendment Flag |
false
|
| Document Period End Date |
Mar. 20, 2025
|
| Entity File Number |
001-35403
|
| Entity Registrant Name |
Verastem,
Inc.
|
| Entity Central Index Key |
0001526119
|
| Entity Tax Identification Number |
27-3269467
|
| Entity Incorporation, State or Country Code |
DE
|
| Entity Address, Address Line One |
117 Kendrick Street
|
| Entity Address, Address Line Two |
Suite 500
|
| Entity Address, City or Town |
Needham
|
| Entity Address, State or Province |
MA
|
| Entity Address, Postal Zip Code |
02494
|
| City Area Code |
781
|
| Local Phone Number |
292-4200
|
| Written Communications |
false
|
| Soliciting Material |
false
|
| Pre-commencement Tender Offer |
false
|
| Pre-commencement Issuer Tender Offer |
false
|
| Title of 12(b) Security |
Common stock, $0.0001 par value per share
|
| Trading Symbol |
VSTM
|
| Security Exchange Name |
NASDAQ
|
| Entity Emerging Growth Company |
false
|
| X |
- DefinitionBoolean flag that is true when the XBRL content amends previously-filed or accepted submission.
| Name: |
dei_AmendmentFlag |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionFor the EDGAR submission types of Form 8-K: the date of the report, the date of the earliest event reported; for the EDGAR submission types of Form N-1A: the filing date; for all other submission types: the end of the reporting or transition period. The format of the date is YYYY-MM-DD.
| Name: |
dei_DocumentPeriodEndDate |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:dateItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe type of document being provided (such as 10-K, 10-Q, 485BPOS, etc). The document type is limited to the same value as the supporting SEC submission type, or the word 'Other'.
| Name: |
dei_DocumentType |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:submissionTypeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 1 such as Attn, Building Name, Street Name
| Name: |
dei_EntityAddressAddressLine1 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionAddress Line 2 such as Street or Suite number
| Name: |
dei_EntityAddressAddressLine2 |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- Definition
+ References
+ Details
| Name: |
dei_EntityAddressCityOrTown |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCode for the postal or zip code
| Name: |
dei_EntityAddressPostalZipCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the state or province.
| Name: |
dei_EntityAddressStateOrProvince |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:stateOrProvinceItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionA unique 10-digit SEC-issued value to identify entities that have filed disclosures with the SEC. It is commonly abbreviated as CIK. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityCentralIndexKey |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:centralIndexKeyItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionIndicate if registrant meets the emerging growth company criteria. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityEmergingGrowthCompany |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionCommission file number. The field allows up to 17 characters. The prefix may contain 1-3 digits, the sequence number may contain 1-8 digits, the optional suffix may contain 1-4 characters, and the fields are separated with a hyphen.
| Name: |
dei_EntityFileNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:fileNumberItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTwo-character EDGAR code representing the state or country of incorporation.
| Name: |
dei_EntityIncorporationStateCountryCode |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarStateCountryItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe exact name of the entity filing the report as specified in its charter, which is required by forms filed with the SEC. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityRegistrantName |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionThe Tax Identification Number (TIN), also known as an Employer Identification Number (EIN), is a unique 9-digit value assigned by the IRS. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b-2
| Name: |
dei_EntityTaxIdentificationNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:employerIdItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionLocal phone number for entity.
| Name: |
dei_LocalPhoneNumber |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:normalizedStringItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 13e-4(c) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 13e
-Subsection 4c
| Name: |
dei_PreCommencementIssuerTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as pre-commencement communications pursuant to Rule 14d-2(b) under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 14d
-Subsection 2b
| Name: |
dei_PreCommencementTenderOffer |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTitle of a 12(b) registered security. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection b
| Name: |
dei_Security12bTitle |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:securityTitleItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionName of the Exchange on which a security is registered. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Number 240
-Section 12
-Subsection d1-1
| Name: |
dei_SecurityExchangeName |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:edgarExchangeCodeItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as soliciting material pursuant to Rule 14a-12 under the Exchange Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Exchange Act
-Section 14a
-Number 240
-Subsection 12
| Name: |
dei_SolicitingMaterial |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionTrading symbol of an instrument as listed on an exchange.
| Name: |
dei_TradingSymbol |
| Namespace Prefix: |
dei_ |
| Data Type: |
dei:tradingSymbolItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
| X |
- DefinitionBoolean flag that is true when the Form 8-K filing is intended to satisfy the filing obligation of the registrant as written communications pursuant to Rule 425 under the Securities Act. Reference 1: http://www.xbrl.org/2003/role/presentationRef
-Publisher SEC
-Name Securities Act
-Number 230
-Section 425
| Name: |
dei_WrittenCommunications |
| Namespace Prefix: |
dei_ |
| Data Type: |
xbrli:booleanItemType |
| Balance Type: |
na |
| Period Type: |
duration |
|
Grafico Azioni Verastem (NASDAQ:VSTM)
Storico
Da Mar 2025 a Mar 2025

Grafico Azioni Verastem (NASDAQ:VSTM)
Storico
Da Mar 2024 a Mar 2025