UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-Q
(Mark One)
☒ QUARTERLY REPORT
PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the quarterly period ended September 30,
2023
or
☐ TRANSITION REPORT
PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from __________ to __________
Commission File Number: 001-36374
ACTINIUM PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
| Delaware | | 74-2963609 |
(State or Other Jurisdiction of
Incorporation or Organization) | | (I.R.S. Employer
Identification No.) |
| | | |
| 100 Park Ave., 23rd Floor New York, NY | | 10017 |
| (Address of Principal Executive Offices) | | (Zip Code) |
(646) 677-3870
(Registrant’s Telephone Number, Including
Area Code)
275 Madison Avenue, 7th Fl.
New York, NY 10016
(Former Address)
Securities registered
pursuant to Section 12(b) of the Act:
| Title of each class | | Trading Symbol | | Name of exchange on which registered |
| Common stock, par value $0.001 | | ATNM | | NYSE American |
Indicate by check mark whether
the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the
preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such
filing requirements for the past 90 days. ☒ Yes No ☐
Indicate by check mark whether
the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T
(§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit
such files). ☒ Yes No ☐
Indicate by check mark whether
the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging
growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting
company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ☐ | Accelerated filer | ☐ |
| Non-accelerated filer | ☒ | Smaller reporting company | ☒ |
| | | Emerging growth company | ☐ |
If an emerging growth company,
indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial
accounting standards, provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether
the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). ☐ Yes ☒ No
Indicate the number of shares
outstanding of each of the issuer’s classes of common stock, as of November 1, 2023: 27,413,441
Actinium Pharmaceuticals, Inc.
Table of Contents
INDEX
PART I - FINANCIAL INFORMATION
ITEM 1. FINANCIAL STATEMENTS
The accompanying consolidated
financial statements have been prepared by the Company and are unaudited. In the opinion of management, all adjustments (which include
only normal recurring adjustments) necessary to present fairly the financial position at September 30, 2023 and December 31, 2022, and
the results of operations and cash flows for the three months and nine months ended September 30, 2023 and 2022, respectively, have been
made. Certain information and footnote disclosures normally included in financial statements prepared in accordance with accounting principles
generally accepted in the United States of America have been condensed or omitted. It is suggested that these financial statements be
read in conjunction with the financial statements and notes thereto included in the Company’s audited financial statements for the
year ended December 31, 2022 in the Company’s Annual Report on Form 10-K. The results of operations for the three months and nine
months ended September 30, 2023 are not necessarily indicative of the operating results for the full year.
Actinium Pharmaceuticals, Inc.
Condensed Consolidated Balance Sheets
(Unaudited)
(amounts in thousands, except share and per share
data)
| | |
September 30,
2023 | | |
December 31,
2022 | |
| | |
(Unaudited) | | |
| |
| Assets | |
| | |
| |
| Current Assets: | |
| | |
| |
| Cash and cash equivalents | |
$ | 82,978 | | |
$ | 108,910 | |
| Restricted cash - current | |
| - | | |
| 396 | |
| Prepaid expenses and other current assets | |
| 2,618 | | |
| 1,636 | |
| Total Current Assets | |
| 85,596 | | |
| 110,942 | |
| | |
| | | |
| | |
| Property and equipment, net of accumulated depreciation of $643 and $487 | |
| 601 | | |
| 604 | |
| Restricted cash – long term | |
| 310 | | |
| 302 | |
| Operating leases right-of-use assets | |
| 2,436 | | |
| 2,341 | |
| Finance leases right-of-use assets | |
| 1 | | |
| 3 | |
| Total Assets | |
$ | 88,944 | | |
$ | 114,192 | |
| | |
| | | |
| | |
| Liabilities and Stockholders’ Equity | |
| | | |
| | |
| Current Liabilities: | |
| | | |
| | |
| Accounts payable and accrued expenses | |
$ | 8,150 | | |
$ | 10,130 | |
| Operating leases current liability | |
| 521 | | |
| 494 | |
| Finance leases current liability | |
| 1 | | |
| 4 | |
| Total Current Liabilities | |
| 8,672 | | |
| 10,628 | |
| | |
| | | |
| | |
| Long-term license revenue deferred | |
| 35,000 | | |
| 35,000 | |
| Long-term operating lease obligations | |
| 1,689 | | |
| 2,083 | |
| Total Liabilities | |
| 45,361 | | |
| 47,711 | |
| | |
| | | |
| | |
| Commitments and contingencies | |
| | | |
| | |
| | |
| | | |
| | |
| Stockholders’ Equity: | |
| | | |
| | |
| Preferred stock, $0.001 par value; 50,000,000 shares authorized, 0 shares issued and outstanding | |
| - | | |
| - | |
| Common stock, $0.001 par value; 1,000,000,000 shares authorized; 27,413,441 and 25,674,823 shares issued and outstanding, respectively | |
| 27 | | |
| 26 | |
| Additional paid-in capital | |
| 371,815 | | |
| 355,220 | |
| Accumulated deficit | |
| (328,259 | ) | |
| (288,765 | ) |
| Total Stockholders’ Equity | |
| 43,583 | | |
| 66,481 | |
| | |
| | | |
| | |
| Total Liabilities and Stockholders’ Equity | |
$ | 88,944 | | |
$ | 114,192 | |
See accompanying notes to the condensed consolidated
financial statements.
Actinium Pharmaceuticals, Inc.
Condensed Consolidated Statements of Operations
(Unaudited)
(In thousands, except share and per share data)
| | |
For the Three Months Ended
September 30, | | |
For the Nine months Ended
September 30, | |
| | |
2023 | | |
2022 | | |
2023 | | |
2022 | |
| Revenue | |
| | |
| | |
| | |
| |
| Revenue | |
$ | - | | |
$ | - | | |
$ | - | | |
$ | - | |
| Other revenue | |
| - | | |
| 45 | | |
| - | | |
| 1,030 | |
| Total revenue | |
| - | | |
| 45 | | |
| - | | |
| 1,030 | |
| | |
| | | |
| | | |
| | | |
| | |
| Operating expenses: | |
| | | |
| | | |
| | | |
| | |
| Research and development, net of reimbursements | |
| 11,622 | | |
| 6,771 | | |
| 30,552 | | |
| 15,802 | |
| General and administrative | |
| 2,729 | | |
| 3,073 | | |
| 11,025 | | |
| 8,041 | |
| Total operating expenses | |
| 14,351 | | |
| 9,844 | | |
| 41,577 | | |
| 23,843 | |
| | |
| | | |
| | | |
| | | |
| | |
| Loss from operations | |
| (14,351 | ) | |
| (9,799 | ) | |
| (41,577 | ) | |
| (22,813 | ) |
| | |
| | | |
| | | |
| | | |
| | |
| Other income: | |
| | | |
| | | |
| | | |
| | |
| Interest income - net | |
| 1,075 | | |
| 325 | | |
| 2,083 | | |
| 443 | |
| Total other income | |
| 1,075 | | |
| 325 | | |
| 2,083 | | |
| 443 | |
| | |
| | | |
| | | |
| | | |
| | |
| Net loss | |
$ | (13,276 | ) | |
$ | (9,474 | ) | |
$ | (39,494 | ) | |
$ | (22,370 | ) |
| | |
| | | |
| | | |
| | | |
| | |
Net loss per common share – basic and diluted | |
$ | (0.49 | ) | |
$ | (0.38 | ) | |
$ | (1.50 | ) | |
$ | (0.94 | ) |
Weighted average common shares outstanding – basic and diluted | |
| 27,058,397 | | |
| 25,164,599 | | |
| 26,329,298 | | |
| 23,691,218 | |
See accompanying notes to the condensed consolidated
financial statements.
Actinium Pharmaceuticals, Inc.
Condensed Consolidated Statement of Changes
in Stockholders’ Equity
For the Period from January 1, 2023 to September
30, 2023
(Unaudited)
(amounts in thousands, except share amounts)
| | |
Common Stock | | |
Additional
Paid-In | | |
Accumulated | | |
Stockholder’ | |
| | |
Shares | | |
Amount | | |
Capital | | |
Deficit | | |
Equity | |
| Balance, January 1, 2023 | |
| 25,674,823 | | |
$ | 26 | | |
$ | 355,220 | | |
$ | (288,765 | ) | |
$ | 66,481 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| - | | |
| - | | |
| 993 | | |
| - | | |
| 993 | |
| Sale of common stock, net of offering costs | |
| 54,414 | | |
| - | | |
| 770 | | |
| - | | |
| 770 | |
| Issuance of common stock from exercise of stock options | |
| 133 | | |
| - | | |
| 1 | | |
| - | | |
| 1 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (11,037 | ) | |
| (11,037 | ) |
| Balance, March 31, 2023 | |
| 25,729,370 | | |
$ | 26 | | |
$ | 356,984 | | |
$ | (299,802 | ) | |
$ | 57,208 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| - | | |
| - | | |
| 1,001 | | |
| - | | |
| 1,001 | |
| Sale of common stock, net of offering costs | |
| 1,210,965 | | |
| 1 | | |
| 9,787 | | |
| - | | |
| 9,788 | |
| Issuance of common stock from exercise of stock options | |
| 44,108 | | |
| - | | |
| 261 | | |
| - | | |
| 261 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (15,181 | ) | |
| (15,181 | ) |
| Balance, June 30, 2023 | |
| 26,984,443 | | |
$ | 27 | | |
$ | 368,033 | | |
$ | (314,983 | ) | |
$ | 53,077 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| 13,144 | | |
| - | | |
| 921 | | |
| - | | |
| 921 | |
| Sale of common stock, net of offering costs | |
| 415,854 | | |
| - | | |
| 2,861 | | |
| - | | |
| 2,861 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (13,276 | ) | |
| (13,276 | ) |
| Balance, September 30, 2023 | |
| 27,413,441 | | |
$ | 27 | | |
$ | 371,815 | | |
$ | (328,259 | ) | |
$ | 43,583 | |
See accompanying notes to the condensed consolidated
financial statements.
Actinium Pharmaceuticals, Inc.
Condensed Consolidated Statement of Changes
in Stockholders’ Equity
For the Three and Nine months Ended September
30, 2022
(Unaudited)
(In thousands, except share amounts)
| | |
Common Stock | | |
Additional
Paid-In | | |
Accumulated | | |
Stockholders’ | |
| | |
Shares | | |
Amount | | |
Capital | | |
Deficit | | |
Equity | |
| Balance, January 1, 2022 | |
| 22,143,974 | | |
$ | 22 | | |
$ | 329,271 | | |
$ | (255,748 | ) | |
$ | 73,545 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| - | | |
| - | | |
| 421 | | |
| - | | |
| 421 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (5,129 | ) | |
| (5,129 | ) |
| Balance, March 31, 2022 | |
| 22,143,974 | | |
$ | 22 | | |
$ | 329,692 | | |
$ | (260,877 | ) | |
$ | 68,837 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| - | | |
| - | | |
| 425 | | |
| - | | |
| 425 | |
| Sale of common stock, net of issuance costs | |
| 2,726,649 | | |
| 3 | | |
| 16,683 | | |
| - | | |
| 16,686 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (7,767 | ) | |
| (7,767 | ) |
| Balance, June 30, 2022 | |
| 24,870,623 | | |
$ | 25 | | |
$ | 346,800 | | |
$ | (268,644 | ) | |
$ | 78,181 | |
| | |
| | | |
| | | |
| | | |
| | | |
| | |
| Stock-based compensation | |
| 19,639 | | |
| - | | |
| 970 | | |
| - | | |
| 970 | |
| Sale of common stock, net of issuance costs | |
| 321,810 | | |
| - | | |
| 1,578 | | |
| - | | |
| 1,578 | |
| Net loss | |
| - | | |
| - | | |
| - | | |
| (9,474 | ) | |
| (9,474 | ) |
| Balance, September 30, 2022 | |
| 25,212,072 | | |
$ | 25 | | |
$ | 349,348 | | |
$ | (278,118 | ) | |
$ | 71,255 | |
See accompanying notes to the condensed consolidated
financial statements.
Actinium Pharmaceuticals, Inc.
Condensed Consolidated Statements of Cash Flows
(Unaudited)
(amounts in thousands)
| | |
For the Nine months Ended
September 30, | |
| | |
2023 | | |
2022 | |
| Cash Flows From Operating Activities: | |
| | |
| |
| Net loss | |
$ | (39,494 | ) | |
$ | (22,370 | ) |
| Adjustments to reconcile net loss to net cash used in operating activities: | |
| | | |
| | |
| Stock-based compensation expense | |
| 2,915 | | |
| 1,816 | |
| Depreciation & amortization expenses | |
| 591 | | |
| 538 | |
| Changes in operating assets and liabilities: | |
| | | |
| | |
| Prepaid expenses and other current assets | |
| (982 | ) | |
| 264 | |
| Accounts payable and accrued expenses | |
| (1,981 | ) | |
| 2,334 | |
| Other revenue deferred – current liability | |
| - | | |
| (907 | ) |
| Long-term license revenue deferred | |
| - | | |
| 35,000 | |
| Operating lease right-of-use assets | |
| (527 | ) | |
| - | |
| Operating lease liabilities | |
| (367 | ) | |
| (253 | ) |
| Net Cash Used In/Provided By Operating Activities | |
| (39,845 | ) | |
| 16,422 | |
| | |
| | | |
| | |
| Cash Flows Used In Investing Activities: | |
| | | |
| | |
| Purchase of property and equipment | |
| (153 | ) | |
| (350 | ) |
| Net Cash Used In Investing Activities | |
| (153 | ) | |
| (350 | ) |
| | |
| | | |
| | |
| Cash Flows Provided By Financing Activities: | |
| | | |
| | |
| Payments on finance leases | |
| (3 | ) | |
| (48 | ) |
| Sales of shares of common stock, net of costs | |
| 13,419 | | |
| 18,264 | |
| Proceeds from the exercise of stock options | |
| 262 | | |
| - | |
| Net Cash Provided By Financing Activities | |
| 13,678 | | |
| 18,216 | |
| | |
| | | |
| | |
| Net change in cash, cash equivalents, and restricted cash | |
| (26,320 | ) | |
| 34,288 | |
| Cash, cash equivalents, and restricted cash at beginning of period | |
| 109,608 | | |
| 78,221 | |
| Cash, cash equivalents, and restricted cash at end of period | |
$ | 83,288 | | |
$ | 112,509 | |
| | |
| | | |
| | |
| Supplemental disclosure of cash flow information: | |
| | | |
| | |
| Cash paid for interest | |
$ | - | | |
$ | - | |
| Cash paid for income taxes | |
$ | - | | |
$ | - | |
See accompanying notes to the condensed consolidated
financial statements.
Actinium Pharmaceuticals, Inc.
Notes to Condensed Consolidated Financial Statements
(Unaudited)
Note 1 - Description of Business and Summary
of Significant Accounting Policies
Nature of Business -
Actinium Pharmaceuticals, Inc. is a biopharmaceutical company developing targeted radiotherapies to deliver cancer-killing radiation with
cellular level precision to treat patients with high unmet medical needs.
Basis of Presentation -
Unaudited Interim Financial Information - The accompanying unaudited interim condensed consolidated financial statements and related
notes have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”)
for interim financial information, and in accordance with the rules and regulations of the United States Securities and Exchange Commission
(the “SEC”) with respect to Form 10-Q and Article 10 of Regulation S-X. Accordingly, they do not include all of the information
and footnotes required by U.S. GAAP for complete financial statements. The unaudited interim condensed financial statements furnished
reflect all adjustments (consisting of normal recurring adjustments) which are, in the opinion of management, necessary for a fair statement
of the results for the interim periods presented. Interim results are not necessarily indicative of the results for the full year. These
unaudited interim condensed consolidated financial statements should be read in conjunction with the audited consolidated financial statements
and notes thereto contained in the Company’s annual report on Form 10-K for the year ended December 31, 2022.
Principles of Consolidation
- The basis of consolidation is unchanged from the disclosure in the Company’s Notes to the Consolidated Financial Statements
section in its Report on Form 10-K for the year ended December 31, 2022. The unaudited condensed consolidated financial statements include
the Company’s accounts and those of the Company’s wholly owned subsidiaries.
Use of Estimates -
The preparation of these unaudited interim condensed consolidated financial statements in conformity with U.S. GAAP requires management
to make estimates and assumptions that affect the reported amounts of assets and liabilities at the date of the consolidated financial
statements and the reported amounts of expenses during the reporting period. Actual results could differ from those estimates.
Cash, Cash Equivalents
and Restricted Cash - The Company considers all highly liquid accounts with original maturities of three months or less to be cash
equivalents. Balances held by the Company are typically in excess of Federal Deposit Insurance Corporation insured limits.
The following is a summary
of cash, cash equivalents and restricted cash at September 30, 2023 and December 31, 2022:
| (in thousands) | |
September 30,
2023 | | |
December 31,
2022 | |
| Cash and cash equivalents | |
$ | 82,978 | | |
$ | 108,910 | |
| Restricted cash - current | |
| - | | |
| 396 | |
| Restricted cash – long-term | |
| 310 | | |
| 302 | |
| Cash, cash equivalents and restricted cash | |
$ | 83,288 | | |
$ | 109,608 | |
Restricted cash relates to
a certificate of deposit held as collateral for a letter of credit issued in connection with the Company’s lease of corporate office
space.
Leases – The
Company has operating and finance leases for corporate office space and office equipment located at the corporate office space. Leases
with an initial term of 12 months or less are not recorded on the balance sheet; lease expense for these leases is recognized on a straight-line
basis over the lease term.
Fair Value Measurement
- Fair value is defined as the price that would be received to sell an asset, or paid to transfer a liability, in an orderly transaction
between market participants. A fair value hierarchy has been established for valuation inputs that gives the highest priority to quoted
prices in active markets for identical assets or liabilities and the lowest priority to unobservable inputs.
Revenue Recognition -
The Company recognizes revenue in accordance with Accounting Standards Codification (ASC) Topic 606, Revenue From Contracts With Customers
(“ASC 606”). Under ASC 606, an entity recognizes revenue when its customer obtains control of promised goods or services,
in an amount that reflects the consideration that the entity expects to receive in exchange for those goods or services. To determine
revenue recognition for arrangements within the scope of ASC 606, the entity performs the following five steps: (i) identify the contract(s)
with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price, including variable
consideration, if any; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue as
the entity satisfies a performance obligation. The Company only applies the five-step model to contracts when it is probable that the
entity will collect the consideration to which it is entitled in exchange for the goods or services it transfers to the customer.
At contract inception, once
the contract is determined to be within the scope of ASC 606, the Company assesses whether the promised goods or services promised within
each contract are distinct and, therefore, represent a separate performance obligation. Goods and services that are determined not
to be distinct are combined with other promised goods and services until a distinct bundle is identified. In determining whether goods
or services are distinct, the Company evaluates certain criteria, including whether (i) the customer can benefit from the good or
service either on its own or together with other resources that are readily available to the customer (capable of being distinct) and
(ii) the good or service is separately identifiable from other goods or services in the contract (distinct in the context of the
contract).
The Company then determines
the transaction price, which is the amount of consideration it expects to be entitled from a customer in exchange for the promised goods
or services for each performance obligation and recognizes the associated revenue as each performance obligation is satisfied. The Company’s
estimate of the transaction price for each contract includes all variable consideration to which it expects to be entitled. Variable consideration
includes payments in the form of collaboration milestone payments. If an arrangement includes collaboration milestone payments, the Company
evaluates whether the milestones are considered probable of being reached and estimates the amount to be included in the transaction price
using the most likely amount method. If it is probable that a significant revenue reversal would not occur, the associated milestone value
is included in the transaction price.
ASC 606 requires the Company
to allocate the arrangement consideration on a relative standalone selling price basis for each performance obligation after determining
the transaction price of the contract and identifying the performance obligations to which that amount should be allocated. The relative
standalone selling price is defined in the revenue standard as the price at which an entity would sell a promised good or service separately
to a customer. The Company then recognizes as revenue the amount of the transaction price that is allocated to the respective performance
obligation as each performance obligation is satisfied, either at a point in time or over time, and if over time, recognition is based
on the use of an output or input method.
Collaborative Arrangements
- The Company follows the accounting guidance for collaboration agreements with third parties, which requires that certain transactions
between the Company and collaborators be recorded in its consolidated statements of operations on either a gross basis or net basis, depending
on the characteristics of the collaborative relationship, and requires enhanced disclosure of collaborative relationships. The Company
evaluates its collaboration agreements for proper classification in its consolidated statements of operations based on the nature of the
underlying activity. When the Company has concluded that it has a customer relationship with one of its collaborators, the Company follows
the guidance of ASC 606.
Grant Revenue –
The Company had a grant from the National Institutes of Health (“NIH”) for research and development related activities
that provided for payments for reimbursed costs, which included overhead and general and administrative costs as well as an administrative
fee. The Company recognized revenue from grants as it performed services under this arrangement. Associated expenses were recognized when
incurred as research and development expense. Revenue and related expenses are presented gross in the consolidated statements of operations.
License Revenue –
The Company entered into a product licensing agreement whereby the Company allowed a third party to commercialize a certain product
in specified territories using the Company’s trademarks. The terms of this arrangement include payment to the Company for a combination
of one or more of the following: upfront license fees; development, regulatory and sales-based milestone payments; and royalties on net
sales of licensed products. The Company uses its judgment to determine whether milestones or other variable consideration should be included
in the transaction price.
Upfront license fees:
If the license to the Company’s intellectual property is determined to be distinct from the other performance obligations identified
in the arrangement, the Company will recognize revenue from upfront license fees allocated to the license when the license is transferred
to the licensee and the licensee is able to use and benefit from the license. For licenses that are bundled with other promises, the Company
determines whether the combined performance obligation is satisfied over time or at a point in time.
Development, regulatory
or commercial milestone payments: At the inception of each arrangement that includes payments based on the achievement of certain
development, regulatory and sales-based or commercial events, the Company evaluates whether the milestones are considered probable of
being achieved and estimates the amount to be included in the transaction price using the most likely amount method. If it is probable
that a significant revenue reversal would not occur, the associated milestone value is included in the transaction price. Milestone payments
that are not within the Company’s or the licensee’s control, such as regulatory approvals, are not considered probable of
being achieved until regulatory approval is received. At the end of each subsequent reporting period, the Company will re-evaluate the
probability of achieving such development and regulatory milestones and any related constraint, and if necessary, adjust the Company’s
estimate of the overall transaction price. Any such adjustments are recorded on a cumulative catch-up basis and recorded as part of license
revenue during the period of adjustment.
Sales-based milestone payments
and royalties: For arrangements that include sales-based royalties, including milestone payments based on the volume of sales, the
Company will determine whether the license is deemed to be the predominant item to which the royalties or sales-based milestones relate
and if such is the case, the Company will recognize revenue at the later of (i) when the related sales occur, or (ii) when the performance
obligation to which some or all of the royalty has been allocated has been satisfied (or partially satisfied).
Upfront payments and fees
may require deferral of revenue recognition to a future period until the Company performs its obligations under these arrangements or
when it is probable that a significant reversal in the amount of cumulative revenue recognized will not occur or when the uncertainty
associated with any variable consideration is subsequently resolved. Amounts payable to the Company are recorded as accounts receivable
when the Company’s right to consideration is unconditional.
Research and Development
Costs - Research and development costs are expensed as incurred. These costs include the costs of manufacturing drug product, the
costs of clinical trials, costs of employees and associated overhead, and depreciation and amortization costs related to facilities and
equipment. Research and development reimbursements are recorded by the Company as a reduction of research and development costs.
Share-Based Payments -
The Company estimates the fair value of each stock option award at the grant date by using the Black-Scholes option pricing model. The
fair value determined represents the cost for the award and is recognized over the vesting period during which an employee is required
to provide service in exchange for the award. The Company accounts for forfeitures of stock options as they occur.
Net Loss Per Common Share
- Basic loss per common share is computed by dividing the net loss available to common stockholders by the weighted average number of
shares of common stock outstanding during the reporting period. For periods of net loss, diluted loss per share is calculated similarly
to basic loss per share because the impact of all potential dilutive common shares is anti-dilutive. For the three and nine months ended
September 30, 2023 and 2022, the Company’s potentially dilutive shares, which include outstanding common stock options, restricted
stock units and warrants, have not been included in the computation of diluted net loss per share as the result would have been anti-dilutive.
| (in thousands) | |
September 30,
2023 | | |
September 30,
2022 | |
| Stock Options | |
| 3,304 | | |
| 3,192 | |
| Restricted Stock Units | |
| 305 | | |
| 300 | |
| Warrants | |
| 1,442 | | |
| 1,443 | |
| Total | |
| 5,051 | | |
| 4,935 | |
Recently Adopted Accounting
Pronouncements – In November 2021, the FASB issued ASU 2021-10, Government Assistance (Topic 832), Disclosures by Business
Entities about Government Assistance, which provides guidance on disclosure requirements to entities other than not-for-profit entities
about transaction with a government that are accounted for by applying a grant or contribution accounting model by analogy. ASU 2021-10
requires an entity to make annual disclosures related to (1) the nature of the transactions and the related accounting policy used to
account for the government transactions, (2) quantification and disclosure of amounts related to the government transactions included
in balance sheet and income statement financial statement line items, and (3) significant terms and conditions of the government transactions,
including commitments and contingencies. The amendments of ASU 2021-10 are effective January 1, 2022, including interim periods. The Company
adopted this standard effective January 1, 2022, and the standard did not have a material impact on the Company’s financial statements.
In October 2021, FASB issued
ASU 2021-08, Business Combinations (Topic 805), Account for Contract Assets and Contract Liabilities from Contracts with Customers,
which provides guidance on accounting for contract assets and contract liabilities acquired in a business combination in accordance with
ASC 606. To achieve this, an acquirer may assess how the acquiree applied ASC 606 to determine what to record for the acquired revenue
contracts. Generally, this should result in an acquirer recognizing and measuring the acquired contract assets and contract liabilities
consistent with how they were recognized and measured in the acquiree’s financial statements. The amendments of ASU 2021-08 are
effective January 1, 2023, including interim periods. The Company will evaluate the impact of ASU 2021-08 on any future business combinations
the Company may enter in the future.
In May 2021, FASB issued ASU
2021-04, Earnings Per Share (topic 260), Debt — Modifications and Extinguishments (Subtopic 470-50), Compensation – Stock
Compensation (Topic 718) and Derivatives and Hedging – Contracts in an Entity’s Own Equity (Subtopic 815-40) – Issuer’s
Accounting for Certain Modifications or Exchanges of Freestanding Equity-Classified Written Call Options, which provides guidance
of a modification or an exchange of a freestanding equity-classified written call option that remains equity classified after modification
or exchange as (1) an adjustment to equity and, if so, the related earnings per share (EPS) effects, if any, or (2) an expense and, if
so, the manner and pattern of recognition. The amendments in this ASU are effective January 1, 2022, including interim periods. The Company
adopted this standard effective January 1, 2022 and the standard did not have a material effect on the Company’s financial statements.
Note 2 - Commitments and Contingencies
On June 15, 2012, the Company
entered into a license and sponsored research agreement with Fred Hutchinson Cancer Research Center (“FHCRC”) to build upon
previous and ongoing clinical trials with apamistamab (licensed antibody). FHCRC has completed both a Phase 1 and Phase 2 clinical trial
with apamistamab. The Company has been granted exclusive rights to the antibody and related master cell bank developed by FHCRC. A milestone
payment of $1 million will be due to FHCRC upon U.S. Food and Drug Administration (“FDA”) approval of the first drug utilizing
the licensed antibody. Upon commercial sale of the drug, royalty payments of 2% of net sales will be due to FHCRC.
Note 3 - Leases
The Company determines if
an arrangement is a lease at inception. This determination generally depends on whether the arrangement conveys to the Company the right
to control the use of a fixed asset for a period of time in exchange for consideration. Control of an underlying asset is conveyed to
the Company if the Company obtains the rights to direct the use of and to obtain substantially all of the economic benefits from using
the underlying asset. The Company has lease agreements which include lease and non-lease components, which the Company has elected to
account for as a single lease component for all classes of underlying assets. Lease expense for variable lease components are recognized
when the obligation is probable. The Company made an accounting policy election to exclude from balance sheet reporting those leases with
initial terms of 12 months or less.
Right-of-use assets and liabilities
are recognized at commencement date based on the present value of lease payments over the lease term. ASC 842 requires a lessee to discount
its unpaid lease payments using the interest rate implicit in the lease or, if that rate cannot be readily determined, its incremental
borrowing rate. As an implicit interest rate was not readily determinable in the Company’s leases, the incremental borrowing rate
was used based on the information available at commencement date in determining the present value of lease payments.
The lease term for all of
the Company’s leases includes the non-cancellable period of the lease plus any additional periods covered by either a Company option
to extend (or not to terminate) the lease that the Company is reasonably certain to exercise, or an option to extend (or not to terminate)
the lease controlled by the lessor. Options for lease renewals were excluded from the lease term (and lease liability) for the Company’s
leases as the reasonably certain threshold were not met.
At September 30, 2023, the
Company has two leases which have been capitalized in accordance with ASC 842, one for corporate office space and one for office equipment.
The Company entered into a lease for corporate office space effective June 1, 2022. The lease has a term of 5 years 2 months, with an
expiration date on July 30, 2027 and current annual rent of $0.6 million. The Company is also responsible for certain other costs, such
as insurance, utilities and maintenance During the nine months ended September 30, 2023, the Company spent $0.5 million on improvements
at its corporate office space, which has been included in the value of the operating right-to-use asset as of September 30, 2023.
The components of lease expense
are as follows:
| | |
Three months ended | | |
Nine months ended | |
| (in thousands) | |
September 30,
2023 | | |
September 30,
2022 | | |
September 30,
2023 | | |
September 30,
2022 | |
| Operating lease expense | |
$ | 173 | | |
$ | 206 | | |
$ | 518 | | |
$ | 440 | |
| | |
| | | |
| | | |
| | | |
| | |
| Finance lease cost | |
| | | |
| | | |
| | | |
| | |
| Amortization of right-to-use assets | |
$ | 1 | | |
$ | 14 | | |
$ | 3 | | |
$ | 54 | |
| Interest on lease liabilities | |
$ | - | | |
$ | - | | |
$ | - | | |
$ | 2 | |
| Total finance lease cost | |
$ | 1 | | |
$ | 14 | | |
$ | 3 | | |
$ | 56 | |
Supplemental cash flow information
related to leases are as follows:
Cash flow information:
| | |
Nine months ended | |
| (in thousands) | |
September 30,
2023 | | |
September 30,
2022 | |
| Cash paid for amounts included in the measurement of lease liabilities: | |
| | |
| |
| Operating cash flow use from operating leases | |
$ | 453 | | |
$ | 302 | |
| Operating cash flow use from finance leases | |
$ | 3 | | |
$ | 2 | |
| Financing cash flow use from finance leases | |
$ | 3 | | |
$ | 48 | |
| | |
| | | |
| | |
| Non-cash activity: | |
| | | |
| | |
| Right-of-use assets obtained in exchange for lease obligations: | |
| | | |
| | |
| Operating leases | |
$ | - | | |
$ | 2,605 | |
| Finance Leases | |
$ | - | | |
$ | - | |
Weighted average remaining lease terms are as follows
at September 30, 2023:
| Weighted average remaining lease term: | |
|
| Operating leases | |
3.8 years |
| Finance Leases | |
0.3 year |
As the interest rate implicit
in the leases was not readily determinable at the time that the leases were evaluated, the Company used its incremental borrowing rate
based on the information available in determining the present value of lease payments. The Company’s incremental borrowing rate
was based on the term of the lease, the economic environment of the lease and reflects the rate the Company would have had to pay to borrow
on a secured basis. Below is information on the weighted average discount rates used at the time that the leases were evaluated:
| Weighted average discount rates: |
|
|
|
|
| Operating leases |
|
|
4.8 |
% |
| Finance Leases |
|
|
8.0 |
% |
Maturities of lease liabilities
are as follows:
(in thousands)
Year ending December 31, | |
Operating
Leases | | |
Finance
Leases | |
| 2023 (excluding nine months ended September 30, 2023) | |
$ | 153 | | |
$ | 1 | |
| 2024 | |
| 618 | | |
| - | |
| 2025 | |
| 630 | | |
| - | |
| 2026 | |
| 643 | | |
| - | |
| 2027 | |
| 380 | | |
| - | |
| Total lease payments | |
$ | 2,424 | | |
$ | 1 | |
| Less imputed interest | |
| (214 | ) | |
| - | |
| Present value of lease liabilities | |
$ | 2,210 | | |
$ | 1 | |
Note 4 - Other revenue
The Company determined that
certain collaborations with a third party are within the scope of ASC 606. The collaboration agreement is made up of multiple modules
related to various research activities. The Company identified a single performance obligation to provide research services within each
module for which the Company receives monetary consideration. The third party can choose to proceed with each module or can terminate
the agreement at any time. The Company recognizes revenue for each module on a straight-line basis over the expected module period. Revenue
for succeeding modules is not recognized until all contingencies are resolved, inclusive of the third party’s ability to terminate
the module. The consideration is recognized as revenue over each module and revenue of $0.9 million was recognized during the nine months
ended September 30, 2022. There was no corresponding revenue recognized from a collaboration during the nine months ended September 30,
2023.
The Company had a grant from
the National Institutes of Health for research and development related activities that provides payments for reimbursed costs, which included
overhead and general and administrative costs, as well as an administrative fee. The Company recognized revenue from grants as it performed
services under this arrangement. Associated expenses are recognized when incurred as research and development expense. Other revenue recognized
from this grant for the nine months ended September 30, 2022 was $0.1 million. There was no corresponding revenue for the nine months
ended September 30, 2023.
On April 7, 2022, the Company
entered into a license and supply agreement (the “License Agreement”) with Immedica Pharma AB (“Immedica”), pursuant
to which Immedica licensed the exclusive product rights for commercialization of Iomab-B (I-131 apamistamab) in the European Economic
Area, Middle East and North Africa (EUMENA) including Algeria, Andorra, Bahrain, Cyprus, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon,
Libya, Monaco, Morocco, Oman, Palestine, Qatar, San Marino, Saudi Arabia, Switzerland, Syria, Tunisia, Turkey, the United Arab Emirates,
the United Kingdom, the Vatican City and Yemen. Upon signing, the Company was entitled to an upfront payment of $35 million from Immedica,
which was received in May 2022. Under the terms of the License Agreement, the Company is eligible to receive regulatory and commercial
milestone payments and is entitled to receive royalties in the mid-20 percent range on net sales of the product in certain countries that
may result from the License Agreement. The Company will continue to be responsible for certain clinical development activities and the
manufacturing of Iomab-B and will retain commercialization rights in the U.S. and rest of the world.
The Company’s contract
liabilities are recorded within Other revenue deferred – current liability or Long-term license revenue deferred in its condensed
consolidated balance sheets, depending on the short-term or long-term nature of the payments to be recognized. The Company’s contract
liabilities primarily consist of advanced payments from licensees. There was no Other revenue deferred – current liability at September
30, 2023 and December 31, 2022. Long-term license revenue deferred was $35.0 million at September 30, 2023 and December 31, 2022; this
deferred revenue will be recognized upon European Union regulatory approval of Iomab-B.
Note 5 - Equity
In August 2020, the Company
entered into the Capital on Demand™ Sales Agreement with JonesTrading Institutional Services LLC, or JonesTrading, pursuant to which
the Company may sell, from time to time, through or to JonesTrading, up to an aggregate of $200 million of its common stock. Shares of
common stock are offered pursuant to a shelf registration statement on Form S-3 filed with the SEC on August 7, 2020. On June 28, 2022,
the Company entered into an Amended and Restated Capital on Demand™ Sales Agreement (the “A&R Sales Agreement”)
with JonesTrading and B. Riley Securities, Inc. (“B. Riley Securities”). The A&R Sales Agreement modifies the original
Capital on Demand™ Sales Agreement to include B. Riley Securities as an additional sales agent thereunder.
For the nine months ended
September 30, 2023, the Company sold 1.7 million shares of common stock, resulting in gross proceeds of $13.8 million and net proceeds
of $13.4 million. For the nine months ended September 30, 2022, the Company sold 3.0 million shares of common stock, resulting in gross
proceeds of $18.9 million and net proceeds of $18.3 million.
Stock Options
The following is a summary
of stock option activity for the nine months ended September 30, 2023:
| (in thousands, except for per-share amounts) | |
Number of
Shares | | |
Weighted
Average
Exercise
Price ($) | | |
Weighted
Average
Remaining
Contractual
Term
(in years) | | |
Aggregate
Intrinsic
Value | |
| Outstanding, January 1, 2023 | |
| 3,396 | | |
$ | 8.00 | | |
| 8.85 | | |
$ | 15,204 | |
| Granted | |
| 166 | | |
| 8.67 | | |
| | | |
| | |
| Exercised | |
| (44 | ) | |
| 5.92 | | |
| | | |
| | |
| Cancelled | |
| (214 | ) | |
| 7.21 | | |
| | | |
| | |
| Outstanding, September 30, 2023 | |
| 3,304 | | |
| 8.12 | | |
| 8.14 | | |
| 1,741 | |
| | |
| | | |
| | | |
| | | |
| | |
| Exercisable, September 30, 2023 | |
| 1,322 | | |
| 11.54 | | |
| 7.41 | | |
| 496 | |
During the nine months ended
September 30, 2023, the Company granted stock options to new employees to purchase 166 thousand shares of common stock with an exercise
price ranging from $6.33 to $11.60 per share, a term of 10 years, and a vesting period of 4 years. The options have an aggregated
fair value of $1.0 million that was calculated using the Black-Scholes option-pricing model. Variables used in the Black-Scholes option-pricing
model include: (1) discount rate range from 3.5% to 4.32% (2) expected life of 6 years, (3) expected volatility range from 80.6% to 81.6%,
and (4) zero expected dividends.
The fair values of all options
issued and outstanding are being amortized over their respective vesting periods. The unrecognized compensation expense at September 30,
2023 was $7.7 million related to unvested options, which is expected to be expensed over a weighted average of 2.7 years. During the nine
months ended September 30, 2023 and 2022, the Company recorded compensation expense related to stock options of $2.4 million and $1.6
million, respectively.
Restricted Stock Units
The following is a summary
of restricted stock unit, or RSU, activity for the nine months ended September 30, 2023:
| (in thousands, except for per-share amount) | |
RSUs | | |
Weighted
Average
Grant date Fair Value
Per Share ($) | |
| Outstanding, January 1, 2023 | |
| 325 | | |
| 5.96 | |
| Granted | |
| 5 | | |
| 8.31 | |
| Cancelled | |
| (25 | ) | |
| 7.31 | |
| Outstanding, September 30, 2023 | |
| 305 | | |
| 5.89 | |
The RSUs vest at the earliest
of a change of control event, the termination of the recipient’s continuous service status for any reason other than by the Company
for cause and the third anniversary of the date of the grant. The fair value of the RSUs, $1.8 million, was determined based on the stock
prices on the dates of the grants and each RSU grant is being recognized over its respective three-year period. The unrecognized compensation
expense at September 30, 2023 of $1.1 million is expected to be expensed over a weighted average of 1.9 years. During the nine months
ended September 30, 2023 and 2022, the Company recorded compensation expense related to RSUs of $0.4 million and $0.1 million, respectively.
Warrants
Following is a summary of
warrant activity for the nine months ended September 30, 2023:
| (in thousands, except for per-share amounts) | |
Number of
Shares | | |
Weighted
Average
Exercise
Price ($) | | |
Weighted
Average
Remaining
Contractual
Term
(in years) | | |
Aggregate
Intrinsic
Value | |
| Outstanding, January 1, 2023 | |
| 1,443 | | |
$ | 16.58 | | |
| 1.33 | | |
$ | 5 | |
| Granted | |
| 2 | | |
| 8.30 | | |
| 10.00 | | |
| | |
| Expired | |
| (3 | ) | |
| 106.80 | | |
| | | |
| | |
| Outstanding, September 30, 2023 | |
| 1,442 | | |
$ | 16.58 | | |
| 0.59 | | |
$ | - | |
| | |
| | | |
| | | |
| | | |
| | |
| Exercisable, September 30, 2023 | |
| 1,437 | | |
$ | 15.79 | | |
| 0.58 | | |
$ | - | |
ITEM 2. MANAGEMENT’S DISCUSSION
AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATION
FORWARD-LOOKING STATEMENT NOTICE
This Form 10-Q contains certain
forward-looking statements. For this purpose, any statements contained in this Form 10-Q that are not statements of historical fact may
be deemed to be forward-looking statements. Without limiting the foregoing, words such as “may,” “will,”
“expect,” “believe,” “anticipate,” “estimate” or “continue” or comparable
terminology are intended to identify forward-looking statements. These statements by their nature involve substantial risks and
uncertainties, and actual results may differ materially depending on a variety of factors, many of which are not within our control. These
factors include but are not limited to economic conditions generally and in the industries in which we may participate; competition within
our chosen industry, including competition from much larger competitors; technological advances and failure to successfully develop business
relationships.
Description of Business
Actinium Pharmaceuticals,
Inc. (“Actinium”) develops targeted radiotherapies intended to meaningfully improve survival for patients with relapsed or
refractory cancer who have failed existing therapies. Our vision is to build a specialty, hospital-focused, radiotherapeutics company
that develops and markets medicines for patients who are treated primarily in large quaternary care hospitals and their catchment areas.
Pipeline Highlights
We intend to leverage the clinical data of our lead product candidates,
Iomab-B and Actimab-A, to potentially improve outcomes in patients with relapsed or refractory acute myeloid leukemia (“r/r AML”)
by launching two radiotherapy drugs over the next several years to address the significant need for better outcomes from treatment with
therapeutics or from undergoing a bone marrow transplant (“BMT”).
We also intend to further
advance Iomab-B beyond acute myeloid leukemia (“AML”) based on promising data as a disease control and conditioning agent
for various other blood cancers. Based on early clinical trial results, we are also working on a lower dose, next generation conditioning
program, Iomab-ACT, for rapidly growing cell and gene therapies.
Our Clinical Pipeline

AML is an aggressive, heterogeneous disease that is difficult-to-treat.
Over 50% of AML patients develop relapsed or refractory disease within one year of being afflicted and have an extremely poor prognosis
and dismal survival. Currently, a BMT is regarded as being able to provide the best treatment outcomes and is the only curative regimen
available for AML patients, however, access is limited to AML patients who are fit enough to withstand the challenges associated with
this treatment. The majority of AML patients are considered not transplantable in routine clinical practice as they are not fit enough
to withstand the rigors of the patient journey, which includes therapy to attain a remission, conditioning regimens to destroy diseased
marrow, challenge of the transplant itself or post-transplant complications.
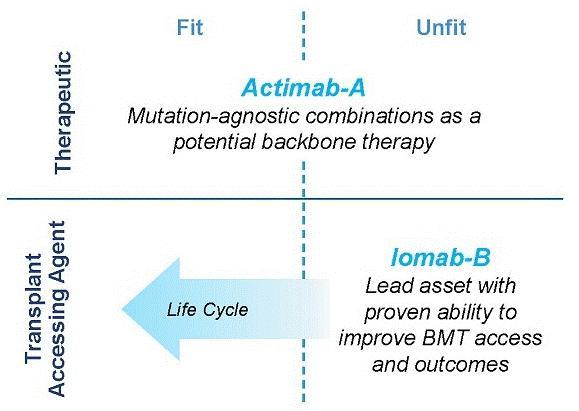
Our Iomab-B and Actimab-A
product candidates have the potential to fill the major unmet medical needs in r/r AML in a complementary fashion as they are directed
at different parts of the patient journey. Iomab-B is being developed as a targeted bridging therapy candidate that we believe could provide
both disease control and conditioning in one agent. We believe results from our Phase 3 SIERRA trial demonstrate the possibility for unprecedented
access to a BMT and improved survival in unfit patients who are currently not considered transplantable in routine clinical practice.
We are developing Actimab-A as a targeted therapy candidate for fit patients. Actimab-A has demonstrated an extension in survival in a
proof-of-concept study and is poised for advanced development in collaboration with the NCI, or National Cancer Institute (“NCI”).
Together, we believe these two product candidates could provide us the opportunity to transform the treatment of AML, especially in the
relapsed and refractory segment which represents over 50% of AML patients.
Iomab-B was evaluated in the
pivotal Phase 3 Study of Iomab-B in Elderly Relapsed or Refractor AML, or “SIERRA trial” with Iomab-B meeting the primary
endpoint of durable Complete Remission (“dCR”) with a high degree of statistical significance (p<0.0001). In February 2023,
we announced full SIERRA trial results, demonstrating unprecedented transplant access and improved outcomes in patients with r/r AML,
with double 1-year and median overall survival (“OS”) compared to control arm patients. These data were presented at the 2023
Tandem Meetings aka the Transplantation & Cellular Therapy (“TCT”) Meetings of the American Society for Transplantation
and Cellular Therapy (“ASTCT”) and the Center for International Blood & Marrow Transplant Research (“CIBMTR”).
We believe these results from the SIERRA trial may provide the opportunity, if we are able to obtain U.S. Food and Drug Administration
(“FDA”) approval, to establish Iomab-B as a potentially new standard of care.
The results from the SIERRA trial have been and are expected to be
presented at the most prestigious and high-impact bone marrow transplant and hematology medical conferences, nuclear medicine conferences
and nursing congresses. This wide exposure is helping broaden the awareness of Iomab-B among members of these relevant medical and scientific
communities as we prepare for potential commercialization subject to FDA approval. Including TCT, the SIERRA Phase 3 results have now been
highlighted in oral presentations at seven international medical conferences in the U.S. and EU attended by key Iomab-B stakeholders including
bone marrow transplant physicians, hematologists and nuclear medicine physicians. Previous and expected Iomab-B SIERRA trial data presentations
include:
| ● | Oral Presentation: European Society for Blood
and Marrow Transplantation (“EBMT”) 49th Annual Meeting, April 2023 |
| | | |
| ● | Oncology Nursing Society (“ONS”)
48th Annual Congress, April 2023 |
| | | |
| ● | Oral Presentation: European Hematology Association
(“EHA”) 2023 Hybrid Congress, June 2023 |
| | | |
| ● | Oral Presentation: Society for Nuclear Medicine
and Molecule Imaging (“SNMMI”) Annual Meeting, June 2023 |
We believe that the medical
and scientific communities present at these events took note of the positive SIERRA clinical trial results, safety and tolerability of
Iomab-B and the successful administration of Iomab-B infusions at various BMT centers, which was done without increasing radiation exposure
risks to treating nursing staff. The SIERRA results were awarded the Henry N. Wagner, Jr., Abstract of the Year award at SNMMI, representing
the top selection out of more than 1,500 abstracts accepted for presentation, which we believe highlights the recognition by the nuclear
medicine community.
Recent Iomab-B SIERRA trial data presentations
include:
| ● | Oral Presentation: European Association of Nuclear
Medicine (“EANM”) 2023 Congress, September 10, 2023 |
| | | |
| ● | Society of Hematologic Oncology
(“SOHO”) 2023 Annual Meeting, September 6, 2023 |
Upcoming Iomab-B SIERRA trial data presentations
| ● | Oral Presentation: American Society of Hematology
Annual Meeting & Exposition, December 10, 2023 |
The data accepted for oral
presentation at ASH on December 10, 2023, will detail survival outcomes of patients with a TP53 mutation enrolled on the SIERRA trial,
highlighting improved survival in patients who received Iomab-B. As disclosed in the ASH abstract published on November 2, 2023, a total
of 37 patients (24.2%) enrolled on the SIERRA trial had a TP53 mutation with 17 patients randomized to the Iomab-B arm and 20 patients
randomized to the control arm of the study. Median Overall Survival for TP53 negative patients receiving Iomab-B was 6.37 months and 5.72
months for TP53 positive patients, demonstrating Iomab-B’s ability to overcome TP53 gene mutations. The median overall survival
of TP53 positive patients on the control arm, including patients who crossed over and received Iomab-B, was 2.96 months. When analyzing
all TP53 positive patients who received Iomab-B, either after initial randomization or crossover, median overall survival was 5.49 months
compared to 1.66 months in patients that did not receive Iomab-B, hazard ratio= 0.23 (p=0.0002).
We are working towards completing
and submitting our Biologics License Application (“BLA”) for Iomab-B to the FDA, and if approved, we intend to commercialize
Iomab-B in the U.S. We have been meeting with the FDA regarding our BLA strategies, and have received positive feedback regarding the
Chemistry, Manufacturing and Controls (“CMC”) package for Iomab-B. The Company, as a continuation of our regulatory interactions
with the FDA, will request a meeting prior to completion of the CMC package to further discuss the clinical and non-clinical modules that
will determine the finalization and timing of our planned BLA filing. As a result of the CMC meeting, as well as updated project timelines
necessitated by the now complete facility modifications at one of our third-party manufacturers, the Company is progressing with completion
of CMC activities and believes it is on track to complete the CMC modules and be in a position to submit a BLA filing in the first half
of 2024. The Early Access Program for Iomab-B is also anticipated to start post completion of these activities. We simultaneously plan
to bring Iomab-B to patients globally and are working with Immedica Pharma AB (“Immedica”), our European, Middle East and
North Africa (“EUMENA”) partner, for the marketing authorization application (“MAA”) of Iomab-B with the European
Medicines Agency (“EMA”). Europe represents a large commercial market opportunity with approximately twice as many transplants
performed in Europe compared to the U.S.
Actimab-A is being developed
under what we believe to be the current industry-leading clinical-study program utilizing the potent alpha radiation emitting isotope
Actinium-225 (“Ac-225”) with clinical data in approximately 150 patients treated over six clinical trials. The potent linear
energy transfer emitted by Ac-225 has no known resistance mechanism. Actimab-A is being developed in combination with other regimens including
chemotherapies and targeted agents to exploit potential mechanistic synergies and leverage the mutation-agnostic mechanism of action of
Ac-225 with the objective of establishing it as a backbone therapy in AML, an extremely heterogenous disease.
We believe our Actimab-A +
CLAG-M therapeutic combination trial results in r/r AML, presented in an oral presentation at ASH in December 2022 validate this approach.
Phase 1 results from the Actimab-A + CLAG-M combination trial showed high response rates and minimal residual disease (“MRD”)
negativity, translating to a survival benefit of 53% and 32% at one and two years in patients who are typically expected to live two to
four months. On September 6, 2023, updated survival data from the Actimab-A + CLAG-M combination trial was presented at SOHO with 30-month
median Overall Survival (“OS”) reported in patients with prior venetoclax treatment who proceeded to BMT and 24-month median
OS in all patients who proceeded to BMT following Actimab-A + CLAG-M treatment. We have also presented Phase 1 data showing that
the combination of Actimab-A + venetoclax was well-tolerated with responses, including a Complete Remission (“CR”) and a partial
response in early dose escalation cohorts. We believe the promise of these results paved the way for the NCI Cooperative Research and
Development Agreement (“CRADA”), announced in February 2023, to develop Actimab-A for the treatment of patients with AML and
other hematologic malignancies. Additionally, we presented the first-ever preclinical data demonstrating the potential synergy of Actimab-A
with FLT3 inhibitors gilteritinib and midostaurin at SOHO. FLT3 is one of the most commonly mutated genes in AML and is associated with
aggressive disease with poor outcomes. Actimab-A was shown to have single-agent activity against FLT3 mutant AML cell lines, supporting
its mutation agnostic mechanism, and enhanced the anti-leukemic activity of the FLT3 inhibition in vitro. We believe these results support
continued evaluation of the combination with the goal of advancing to clinical trials. Based on this data update, Actinium expects to
initiate the late-stage development of Actimab-A, including a potential pivotal trial, in combination as a backbone therapy for r/r AML
under the CRADA with the NCI and the NCI expects to meet with the FDA in the first quarter of 2024 to finalize a pivotal trial design.
To explore the potential for
a broader development opportunity with our Actimab-A program, we are studying the potential use of Actimab-A in solid tumor indications
through our R&D efforts. CD33-expressing myeloid derived suppressor cells (“MDSCs”) are present within the tumor microenvironment
and exert immunosuppressive effects. In April 2023, we presented preclinical data at the Association for Cancer Research (“AACR”)
Annual Meeting that depicted Actimab-A’s role in the tumor microenvironment to overcome immunosuppression driven by MDSCs. We believe
that our findings thus far show Actimab-A’s potential to selectively deplete MDSCs in lung and colorectal cancer. Actimab-A also
demonstrated superior depletion of human MDSCs compared to Mylotarg, a CD33-targeted antibody-drug conjugate (“ADC”) in colorectal
cancer (p<0.01), highlighting the powerful cytotoxicity and potential therapeutic benefit of radiotherapy compared to naked antibodies
or ADCs. Additional preclinical data evaluating Actimab-A for the targeting of MDSCs has been accepted for presentation at the Society
of Immunotherapy of Cancer (“SITC”) 38th Annual Meeting on November 4, 2023. We believe that the data we have
gathered to-date continues to support our objective to demonstrate the potential for Actimab-A to be a backbone therapy to broadly improve
antitumor activity of immunotherapies and other therapeutic modalities.
Our differentiated R&D
efforts are further exemplified by our next-generation Iomab-ACT conditioning program for rapidly growing cell and gene therapies, as
well as our solid tumor and immunotherapy collaborations with Astellas Pharma Inc. (“Astellas”), AVEO Oncology/LG Chem (“LG
Chem”) and EpicentRx, Inc. (“EpicentRx”). We have several ongoing programs in solid tumors at the pre-clinical stage
with investigational new drug (“IND”) enabling studies underway.
Our platform has been
used to develop a pipeline of novel radiotherapeutic assets to drive company growth. Preclinical pharmacology studies with our
targeted radiotherapeutics directed at validated cancer targets including HER3, HER2, CD33 and CD38, have shown strong improvement
in tumor growth inhibition in various preclinical tumor models as single agents or in combination with targeted agents and
immunotherapy such as checkpoint inhibitors including magrolimab, an anti-CD47 monoclonal antibody. These results have prompted our
team to spearhead efforts in multiple solid tumor programs.
Our intellectual property
(“IP”) portfolio includes over 220 issued patents and pending patent applications worldwide.
With approximately $82.9 million
cash on hand as of September 30, 2023, we expect to fund operations through 2025 as we continue to drive ahead in executing our strategy
to realize our vision.
Market Opportunity
The market opportunity for
Iomab-B and Actimab-A, as depicted in the diagram below, exists in AML and for cellular therapy conditioning in various blood cancers.
We believe that Iomab-B and Actimab-A can fill the major unmet medical needs in r/r AML in a complementary fashion as they are utilized
in different parts of the patient treatment journey. The incidence of AML is approximately 21,000 patients per year, with a prevalence
of approximately 70,000 in the U.S., (approximately 27,500 new patients per year in Europe) and the disease has an outsized economic impact
relative to its population size. Over 50% of patients diagnosed with AML will develop relapsed or refractory disease, with a median age
of 68 years at diagnosis. Despite 11 new approved therapies since 2017, no significant advancements have been made toward a cure and there
is an important unmet medical need for better therapeutics, which provide the opportunity for Actimab-A. Actimab-A is a targeted radiotherapy
for fit patients that has demonstrated an impressive improvement in survival in a proof-of-concept study and is poised for advanced development
in collaboration with the NCI. Using Actimab-A in combination with chemotherapy or a targeted therapy, we have the potential opportunity
to treat both newly diagnosed or r/r AML patients, with the potential addressable population comparable to the prevalence of patients
with AML.

Today, less than 20% of all
AML patients and less than 5% of r/r AML patients are able to access a BMT, currently the only potentially curative option. Most patients
receiving BMT are fit, in remission and able to withstand the challenges associated with this treatment, leaving the large majority of
AML patients ineligible for transplant. This provides an opportunity for Iomab-B, which has demonstrated the ability to enable unfit patients
to benefit from a BMT. Thus Iomab-B can potentially expand the market from the approximately 400 r/r AML patients who are transplanted
currently to approximately 8,000 unfit patients that could be eligible for transplant. Iomab-B has also demonstrated the ability to improve
BMT access with extended survival and potentially curative outcomes in several other hematological diseases outside of AML. Several clinical
trials in over 300 patients with myelodysplastic syndromes (“MDS”), acute lymphocytic leukemia (“ALL”), Hodgkin’s
lymphoma (“HL”), Non-Hodgkin lymphoma (“NHL”) and multiple myeloma (“MM”) have demonstrated the same
value proposition as in AML. This data provides a potential opportunity to expand the market for Iomab-B beyond AML via label expansion.
In the U.S., there are approximately 185,000 patients diagnosed annually with blood cancers (e.g., leukemia, lymphoma, and myeloma) that
are treatable with BMT, of which, approximately 20,000 are transplanted, leaving greater than 165,000 patients who could potentially benefit
from transplant. These patients do not receive a BMT today primarily because they are unfit with active disease and are not considered
eligible, as they cannot tolerate the rigors of therapy required to induce a remission and the conditioning agents required to ablate
the marrow prior to a BMT.
Beyond BMT, the opportunity
exists for better conditioning in other areas of cellular therapy such as CAR-T as well as gene therapies. The pipeline of CAR-T and gene
therapies has rapidly expanded, with the addressable patient population expected to nearly double in the next one to five years and reach
approximately 93,000 patients in the U.S. by 2030 based on the current pipeline of cellular therapies. The CAR-T market size in terms
of dollars is estimated to grow at a CAGR of approximately 11% over the next 5 plus years. The addressable market for Iomab-ACT is in
line with the patient population for cellular therapy as all patients receive conditioning of some type prior to these treatments. We
will continue to develop Iomab-ACT, our lower dose, next generation conditioning program for rapidly growing cell and gene therapies based
on early promising results, ultimately with the value proposition of improving overall access and outcomes for patients who need cellular
or gene therapies.
Our Strategy
Actinium’s strategy
is to build a fully integrated, specialty radiotherapeutics company focused on the top 100 cancer hospitals using the power of our platform
to deliver new treatment options for patient populations living with high unmet medical needs in hematology and oncology. We believe our
focus on relapsed or refractory disease in cancer indications with high unmet medical need, with limited or no competition, and where
the primary delivery of care occurs in large comprehensive cancer care centers, is the appropriate strategy for our company. The cell
killing power of linear energy transfer delivered via radiotherapeutics is unmatched by other technologies and we believe relapsed/refractory
disease is an area where radiotherapeutics can succeed over other approaches. However, radiotherapeutics must be delivered on a just-in-time
basis, and commercial and supply chain barriers are higher than with other types of medicines. The validity of our approach is demonstrated
by our product development strategy as well as the commercial and operating model that we are building for our lead product candidates,
Iomab-B and Actimab-A.
We intend to transform the
treatment of AML with our Iomab-B and Actimab-A product candidates, each of which has demonstrated extension of survival in the most difficult-to-treat
patients who are typically expected to survive for two to four months. The r/r AML segment comprises over 50% of all AML patients. Actimab-A,
a therapeutic agent, and Iomab-B for induction and conditioning, can be used in a complementary fashion as depicted in the diagram below.
Based on the clinical evidence with these product candidates, we intend to develop and commercialize these two radiotherapy drugs, starting
with Iomab-B and followed by Actimab-A, if approved, with the goal of improving survival in patients with r/r AML.
Iomab-B and Actimab-A have the potential to significantly improve
r/r AML outcomes in a complementary manner
The operating model
required to achieve our vision is attractive for several reasons, including the concentrated point of care; the top 50 transplant
centers account for approximately 75% of BMTs and the top 100 hospitals treat over 50% of r/r AML patients. Further, there is
significant overlap in the healthcare providers and ecosystem required to diagnose, treat and care for r/r AML patients within these
hospitals, which we believe will enable us to deploy a relatively small commercial organization and operate an appropriately sized
supply chain.
Our product pipeline is targeting
a broader opportunity in conditioning via label expansion of Iomab-B into BMT for other blood cancers and with Iomab-ACT, our next generation
conditioning program for rapidly growing cell and gene therapies. Further, our solid tumor programs are initially directed at r/r cancers,
a stage of disease where treatment is again concentrated in large hospitals, which account for a significant portion of patients. We believe
our strategy will enable us to build a successful company with high operating efficiencies and is feasible to achieve without requiring
a commercial partner.
Our strategic priorities are to:
| |
● |
Establish
Iomab-B as the standard of care to improve BMT access and survival outcomes in r/r AML patients
who are currently not considered transplantable in routine clinical practice: We
intend to file a BLA in the first half of 2024 based on the positive results from the Pivotal
Phase 3 SIERRA trial and successful regulatory interactions with the FDA. We intend to leverage
our operating track record at key cancer centers to build an organization that can effectively
commercialize Iomab-B. By virtue of the SIERRA trial, we have established operations at 24
leading BMT centers in the U.S (22) and Canada (2) that represent about 30% of transplant
volume and have strong working partnership with Key Opinion Leaders (“KOLs”)
and their teams. The SIERRA results demonstrating unprecedented access to BMT and outcomes
along with our commitment to operational excellence provides a strong foundation for our
commercial team in the U.S. We will also work with our partner Immedica to support the MAA
for the EU and support Iomab-B’s potential approval and launch with our expertise,
as well as supply drug product for commercialization. |
| |
● |
Advance Actimab-A in combinations as a backbone therapy for r/r AML: We intend to progress late-stage development of Actimab-A to leverage its mutation-agnostic mechanism of action (“MOA”) and exploit synergies in combination with other treatments to develop it as an AML backbone therapy. This approach is validated by proof-of-concept data from our Actimab-A + CLAG-M combination trial in r/r AML, which included 57% of patients who had failed venetoclax and are expected to live two to four months on average. The results demonstrated high response rates overall and in these venetoclax failed patients’ median OS was 59% at one year and 32% at two years. Our collaboration with the NCI under the CRADA could provide broad support for late-stage development of Actimab-A + CLAG-M and also other clinical trials to broaden use of Actimab-A. Actimab-A, if approved, would enable us to launch a second product that is complementary to Iomab-B and fulfill our ambition of transforming the treatment outcomes of r/r AML and expand our commercial footprint into the remaining top 100 cancer care centers outside of the leading BMT hospitals. |
| |
● |
Expand the Iomab-B label and revenue stream via life cycle management: We intend to leverage data from several clinical trials that demonstrate the ability of Iomab-B to improve BMT access and outcomes in five additional hematologic indications. These data in MDS, ALL, HL, NHL and MM provide the foundation to expand the label for Iomab-B and increase its market potential. In AML, we would seek label expansion into haploidentical transplants, earlier lines of treatment and younger patients below the age of 55, the cutoff in the SIERRA trial. As much as possible, we would seek to use investigator sponsored trials as the primary strategy for label expansion in order to maximize capital utilization. |
| |
● |
Further expand our conditioning franchise by developing Iomab-ACT for cell and gene therapies: We plan to develop Iomab-ACT to be used for either lymphodepletion or reduced intensity conditioning prior to CAR-T and gene therapies. Similar to BMT, access and outcomes of patients who might benefit from these therapies is currently limited by sub-optimal chemotherapy-based conditioning agents. The number of patients potentially eligible for Iomab-ACT is growing with increased availability of commercial cell and gene therapy products, as well as the expanding number of indications. We are studying Iomab-ACT in conditioning prior to CAR-T cellular therapy via a National Institutes of Health (“NIH”) grant that was recently extended to the Phase 2 portion to fund the ongoing clinical trial with Memorial Sloan Kettering Cancer Center (“MSKCC”). We expect to present proof-of-concept data from this study and announce further development of this program in the CAR-T space by the end of 2023. |
| |
● |
Leverage our R&D capabilities
and technological prowess to advance our solid tumor programs and partnerships: We intend
to continue to direct our R&D effort to advance our solid tumor programs into the clinic and
support life cycle management for Iomab-B and Actimab-A. Our solid tumor programs and technological
capabilities are validated by our partnerships with Astellas, LG Chem, and EpicentRx. Our R&D
capability is demonstrated by our patent portfolio with over 220 issued and pending patent applications
worldwide which include protection for Iomab-B into 2037. Our IP portfolio also includes several
patent families to manufacture Ac-225 in a cyclotron and includes valuable know-how. |
| |
● |
In keeping with our strategic vision over the next five years, we plan to first focus on ensuring an Iomab-B approval and successful launch into core BMT centers to support commercial success. We intend to expand the Iomab-B label and revenue stream while progressing the development of Actimab-A by leveraging the NCI CRADA. We will progress the development of Iomab-ACT to proof-of-concept and explore potential partnerships as a means to achieve commercialization. Our solid tumor programs will progress toward the clinic as we continue to build out our commercial footprint into the top 100 hospitals leaving us positioned to develop them in line with our vision. With commercial dynamics aligning favorably for a successful Iomab-B launch and with late-stage development of Actimab-A in collaboration with the NCI, we plan to deliver on our mission to transform the treatment of AML and patient outcomes, and create a highly differentiated, specialty radiotherapeutics company focused on the top 100 large hospitals. |
Our Product Pipeline
We have strategically focused
our development efforts in areas where there is a significant unmet medical need. We are developing a portfolio of novel radiotherapeutics
that has the potential to positively impact the outcomes of people living with hard-to-treat diseases such as r/r AML via both a therapeutic
and induction/conditioning agent. Outside of AML, our pipeline development offers the opportunity to enhance the value proposition of
cell and gene therapies with our targeted conditioning programs.

AML Focused Programs – Iomab-B
and Actimab-A
Our Iomab-B and Actimab-A
product candidates are focused on addressing the major unmet medical needs in r/r AML in a complementary manner and are directed at different
parts of the patient journey.
Iomab-B – Targeted Radiotherapeutic
for Induction and Conditioning. A potential new standard of care enabling a curative BMT in currently non-transplantable r/r AML patients
with poor survival prognosis
Opportunity to Change the Current Paradigm
for Accessing a BMT and Improving Outcomes
The current approach in
preparing patients for a BMT is to first induce a remission with therapeutic agents to reduce the disease burden and then suppress
or destroy the patient’s immune system, including the diseased bone marrow, with conditioning regimens prior to transplanting
the healthy donor hematopoietic stem cells, which are expected to restore normal bone marrow function following engraftment. As this
approach requires patients to withstand multiple challenges from non-targeted therapies, which include chemotherapy agents and/or
total body irradiation that are highly toxic, BMT is typically limited to FIT patients. Iomab-B is a targeted therapy that provides
both disease control (induction) and conditioning in one agent and is well-tolerated even by UNFIT patients who typically are not
transplanted in routine practice today. The SIERRA trial was designed to demonstrate that UNFIT patients with active disease could
be administered Iomab-B and proceed directly to a BMT without the need for inducing a remission and that this approach could result
in improved survival and curative outcomes. As seen by the positive results of the SIERRA trial detailed below, Iomab-B represents
an exciting new potential paradigm in the management of AML patients and establishes a potential new standard of care especially for
UNFIT patients in the relapsed or refractory setting.
A similar approach has also
been tried in the Phase 3 ASAP trial but with FIT patients. However, to avoid confusion between the potential of the approaches used in
the ASAP and SIERRA trials, important distinctions between these trials are depicted in the graphic below. The ASAP trial sought to demonstrate
non-inferiority between two non-novel approaches and found that outcomes similar to those of current practice could be achieved without
first getting a patient into remission before taking them to BMT by giving them sequential conditioning or treating them twice with non-targeted
chemotherapy agents that are typically used in this setting.
The ASAP approach is limited
to only FIT patients as the UNFIT patients treated in SIERRA could not tolerate ASAP’s highly toxic sequential conditioning approach.
Sequential conditioning is not novel as a similar trial to ASAP was conducted by the UK National Cancer Research Institute in 2019, which
did not show any benefit from this approach in high-risk AML and MDS patients (Craddock et al. Augmented Reduced Intensity Regimen Does
Not Improve Post allogeneic Transplant Outcomes in Acute Myeloid Leukemia. J Clin Oncol. 2021). The SIERRA trial results therefore
can change the paradigm in transplant because non-transplantable patients in routine clinical practice can benefit from a transplant with
Iomab-B and have superior outcomes. While both approaches in these trials support increased access to BMT, only Iomab-B is applicable
to the unfit patients who comprise approximately 80% of r/r AML patients and can potentially expand the market for transplant.

Schetelig et al. Results from the Randomized
Phase III ASAP Trial. ASH 2022
Pivotal Phase 3 SIERRA Trial for Iomab-B (131Iodine-apamistamab)
The SIERRA trial was designed
to demonstrate the ability of Iomab-B to overcome challenges related to patient access to curative BMT. Unfortunately, approximately 30%
of patients with AML have primary refractory disease while approximately 50% relapse quickly after achieving initial remission. Getting
these patients with primary r/r AML into remission is very challenging due to characteristics such as age, comorbidities, and disease
features such as high-risk mutations that contribute to lack of response to salvage therapies and limit treatment options.
Patients must be able to overcome
several challenges related to curative BMT. The first access challenge is that the patient needs to be in complete remission prior to
BMT. The current clinical practice is not to transplant patients with active AML as outcomes are poor due to high relapse rates. The National
Comprehensive Cancer Network (“NCCN”) guidelines also recommend treatment to achieve remission prior to transplant in patients
with relapsed AML. The second challenge to access is tolerance to current conditioning regimens. For older patients, myeloablative regimens
are not an option due to intense toxicity and mortality. The third challenge is the ability to achieve post-BMT remission and successful
engraftment. Inadequate conditioning can lead to graft failure, which is associated with very high mortality. Patients who fail to achieve
a CR post-transplant have extremely poor outcomes and a survival of a few weeks. The fourth challenge relates to BMT tolerability and
post-BMT complications. The conditioning and immunosuppressive regimens given to these patients put them at high risk for infectious complications
and toxicity. In the SIERRA trial, Iomab-B addressed all four of these challenges. Access to BMT is improved as CR is not needed pre-BMT
given effective disease control and targeted myeloablation. With better post-BMT engraftment, CR and lower complications, the SIERRA trial
also addressed the challenges related to improved outcomes through Iomab-B.
The SIERRA results, presented
in the late-breaker session at the 2023 Tandem Meetings: Transplantation & Cellular Therapy Meetings of the ASTCT and the CIBMTR,
support Iomab-B’s value proposition of enabling both improved access and outcomes of a BMT, thereby providing a significant curative
option for r/r AML patients, a segment that represents approximately 50% of all AML patients and the majority not transplanted today.
The design of the SIERRA trial is provided in the figure below.
SIERRA: A Novel, Pivotal Phase 3 Study of
Iomab-B in r/r AML

The pivotal Phase 3 SIERRA
trial was a 153-patient, randomized, multi-center, controlled trial of Iomab-B in patients aged 55 and above with active r/r AML, who
were heavily pre-treated and had high-risk characteristics. Patients enrolled had blast counts of 5% or greater in the marrow or circulating
blasts suggestive of active AML. In this study, Iomab-B was compared to the control arm that allowed physician’s choice of over
20 available agents, including chemotherapies and/or targeted therapies such as venetoclax (BCL-2 inhibitor), FLT3 inhibitors, IDH inhibitors
and Mylotarg, reflecting current best treatment practices attempting to get patients to CR. The control arm included recently approved
AML therapies that were added to the SIERRA protocol as they became available. The crossover arm was designed in SIERRA for an equipoise
that offered Iomab-B to patients failing to achieve a CR on the control arm with an intent to rescue them by taking them to transplant.
Of note, SIERRA had highly restrictive optionality for post-transplant maintenance. Patients with active, r/r AML are not considered eligible
for BMT with current approaches and the SIERRA trial was the only randomized Phase 3 trial to offer BMT as a treatment option for this
patient population. These patients would not be offered BMT in standard practice and therefore have dismal survival outcomes of two to
three months. The primary endpoint of the SIERRA trial was dCR of 6-months and the secondary endpoints are OS and Event-Free Survival
(“EFS”). The comparison of OS in subjects randomized to the control arm who crossed over to receive Iomab-B versus all others
in the control group was an exploratory efficacy endpoint.
As seen in the graphic below,
the primary endpoint of 6-month dCR was met with a high degree of statistical significance (p<0.0001). 75% of patients (44/59) receiving
Iomab-B achieved an initial remission 30 days after their BMT compared to 6.3% of patients (4/64) in the control arm. 22% of the patients
receiving Iomab-B maintained dCR lasting 6-months or more despite limited optionality for post-transplant maintenance, while none of the
patients on the control arm achieved dCR. The current standard practice is to administer post-transplant maintenance therapy to reduce
chances of relapse. The results presented below are on a per protocol basis, which means that only data that was in strict adherence to
the protocol without any deviations was considered for the analysis. It is important to note that the p-value of the primary endpoint
in the Intent-to-Treat (“ITT”) analysis was <0.0001, the same as the per protocol analysis.
SIERRA Results: Iomab-B Meets Primary Endpoint
with High Significance (p<0.0001)
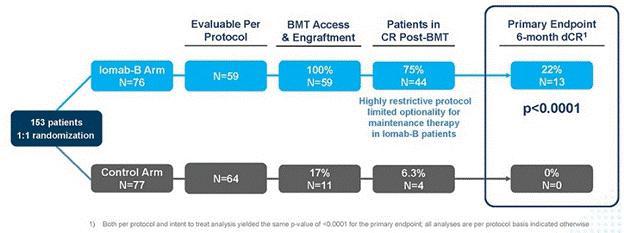
As demonstrated in the OS
graph below, patients who achieved 6-month dCR had 92.3% 1-year survival and 59.9% 2-year survival. Median OS had not been reached in
these patients. It is worth noting that two years in CR is a significant milestone in this patient population, highly indicative of long-term
survival and a possible curative outcome.
Overall Survival for Patients who Achieved
6-month dCR with Iomab-B
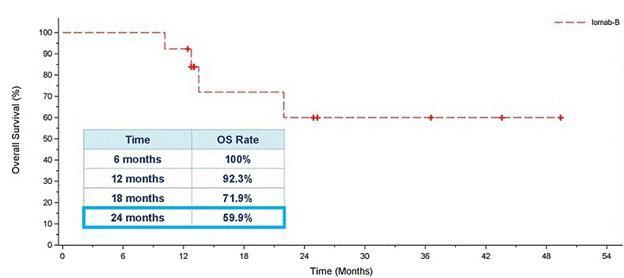
OS was one of the secondary
endpoints of the study. The Kaplan-Meier plot in the inset of the graph below shows ITT OS results between the Iomab-B arm and the control
arm. Due to the crossover design, ITT analysis of OS was confounded by the early crossover of patients (within 28 days) from the control
arm to the Iomab-B arm (57.1%). The effective rescue of these crossover patients by Iomab-B led to an outsized contribution of the Iomab-B
effect on control arm patients. As a result, median OS in the Iomab-B arm was similar to that in the control arm and this secondary endpoint
was not met in the ITT analysis.
In order to isolate the true
impact of Iomab-B on OS, one of the exploratory efficacy endpoints was the comparison of OS in subjects randomized to the control arm
who crossed over to receive Iomab-B versus all others in the control arm, as well as the control arm patients who did not crossover versus
the Iomab-B arm. The Kaplan-Meier plot of OS in the graphic below shows that this exploratory analysis demonstrated the clear benefit
of Iomab-B over the control arm. The median OS for the Iomab-B group was 6.4 months which was double the 3.2 months for the non-crossover
patients in the control arm. Patients who crossed over from the control arm to receive Iomab-B had a median OS of 7.1 months demonstrating
further the ability of Iomab-B to treat patients who are non-treatable by conventional means.
A similar pattern favoring
the Iomab-B group was seen across the pre-defined subgroups, where 1-year OS for Iomab-B was 26.1% compared with 13.1% for the non-crossover
control arm. The 1-year OS for patients in the crossover arm was 35.8%. This clearly demonstrates the OS benefit of Iomab-B over the control
arm and two to three-fold improvement in survival outcomes possible with its use.
Kaplan-Meier Plot of Overall Survival ‒
Iomab-B, Crossover, and Non-Crossover Control Arm

Iomab-B produced a significant
and clinically meaningful improvement in the secondary endpoint of EFS, with a 78% reduction in the probability of an event (Hazard Ratio=0.22,
p<0.0001 for both per protocol and ITT basis). EFS at 6-months for the Iomab-B arm was 28% compared to 0.2% for the control arm. In
the SIERRA trial, an event is defined as one of the following: a patient not achieving CR/CRp or crossing over, patient not receiving
BMT, or a patient relapse or death.
In the figure below comparing
EFS with Iomab-B versus the control arm, the initial vertical drop in the curve in the Iomab-B arm represents those patients who did not
achieve a remission after Iomab-B or those who did not proceed to transplant, while the initial vertical drop in the curve in the control
arm mainly represents patients who did not achieve a remission with salvage therapy and either crossed over to Iomab-B or went onto best
supportive care.
Event-Free Survival with Iomab-B Versus Control
Arm
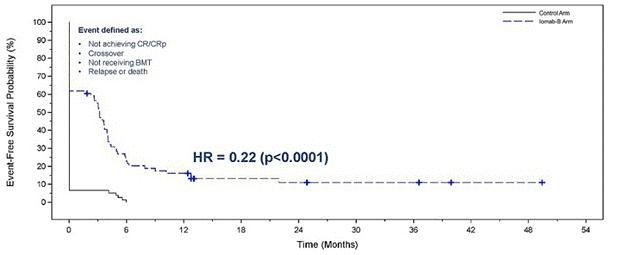
The table below shows relevant
adverse events in transplanted Iomab-B patients. In these patients, incidence of sepsis was four times lower in the Iomab-B arm than the
control arm (6.1% vs. 28.6%). In addition, rates of other treatment related adverse events were lower in favor of Iomab-B, including febrile
neutropenia (43.9% vs. 50.0%), mucositis (15.2% vs. 21.4%) and acute graft versus host disease (“GVHD”) (26.1% vs. 35.7%).
Grade ≥3 Treatment-Emergent Adverse Events
in Transplanted Patients Through Day 100 Post-HCT
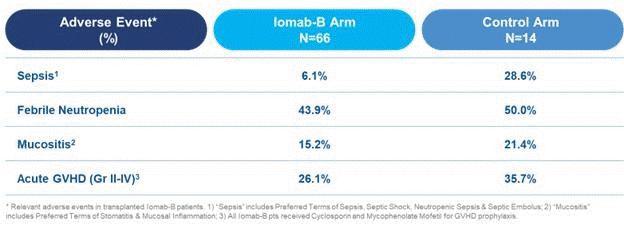
With current treatment practice,
patients who have r/r AML with active disease, utilizing current conditioning agents have poor outcomes and very low survival rates. Using
an Iomab-B led regimen, an unprecedented number of patients were able to access transplant and were able to do so with active disease,
eliminating the need for achieving a CR in order to transplant the patient. Thus, patients are also able to access BMT faster with Iomab-B,
in less than half the time compared to conventional care. Iomab-B represents an exciting new paradigm with the potential to establish
a new standard of care in r/r AML setting, making it possible for most patients to get to a successful transplant with Iomab-B, with a
portion of these patients having a long-term survival benefit. As shown below, with an Iomab-B led regimen, the majority of patients who
are non-transplantable in routine clinical practice can be successfully transplanted, administering myeloablative radiation with reduced
intensity conditioning tolerability to ultimately achieve transformative survival outcome, changing the treatment paradigm for r/r AML
patients.
Iomab-B – New Paradigm to Upend BMT
Access and Improve r/r AML Outcomes
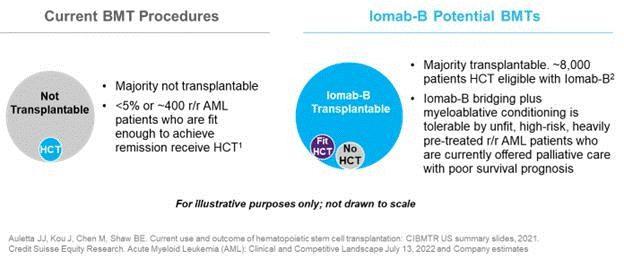
Future Development and Life Cycle Management
for Iomab-B
The results of the Pivotal
Phase 3 SIERRA trial validate the value proposition of Iomab-B, and we believe it could establish unprecedented access to transplant (currently
the only curative option) with better safety and tolerability and improved outcomes, all of which could potentially make Iomab-B the new
standard of care for patients with r/r AML.
We intend to commercialize
Iomab-B in the U.S. The commercial opportunity is supported by favorable dynamics, summarized by the “Three Ps and Two Cs”:
| |
● |
Patients: With its promising profile, Iomab-B provides the opportunity for unprecedented BMT access and better outcomes for patients, with favorable safety and tolerability |
| |
● |
Physicians: Our goal is to help physicians make BMT an option for a vast majority of r/r AML patients who currently are unable to access transplant without disruption to current practice. Patients are able to return to their referring physicians for post-BMT follow-up, and long-term care |
| |
● |
Payers: Iomab-B potentially unlocks value through getting patients safely to effective, potentially curative transplants, with improved outcomes and a manageable safety and tolerability profile |
| |
● |
Competition: While there have been multiple new product approvals in AML over the last several years, they primarily focus on addressing genetic mutations, with limited competition in conditioning to increase access to BMT. We do not see direct or indirect visible competition for Iomab-B in the 5-to-10-year horizon to impair the commercial success of Iomab-B |
| |
● |
Concentrated Call Points: The commercialization for Iomab-B will benefit from a concentrated market. The top 50 centers perform 75% of BMTs and tend to be concentrated in metropolitan areas. These factors allow for commercialization delivered by a focused 35–50-person commercial organization. |
The favorable commercial dynamics
for Iomab-B in the U.S. are further supported by the strong foundation of core competencies developed during the successful execution
of the SIERRA trial at leading high-volume BMT centers. We established and actively managed an end-to-end supply chain, never missing
a patient dose, and were able to treat 60% more patients than expected due to the high number of crossover patients. We focused on operational
excellence at the point of care, working in partnership with leading KOLs and their teams to successfully execute SIERRA at a wide array
of centers. As a result, we have broad reach across leading BMT centers that account for 30% of BMT volume, which speaks to the concentration
of the BMT market. The positive SIERRA results of unprecedented access and outcomes along with our commitment to operational excellence
provide a strong foundation for our commercial team.
In April 2022, Actinium licensed
the EUMENA commercial rights for Iomab-B to Immedica, an independent pharmaceutical company headquartered in Sweden. Immedica has significant
know-how and experience in commercializing niche and specialty care products across Europe and the Middle East, with extensive regulatory
and commercial expertise and capabilities. Actinium will continue to be responsible for certain clinical development activities and Iomab-B
manufacturing and will retain commercialization rights in the U.S. and rest of the world. Currently, there an estimated ~7,200 BMTs for
AML in EUMENA, two times that of the U.S., performed in a concentrated number of centers. The incidence rate of AML in Europe is 3.7 per
100,000, or ~27,500 new patients per year. Actinium received an upfront payment of $35 million USD with the potential for an additional
$417 million USD in regulatory and sales milestones and mid-twenty percent royalties. Iomab-B has been granted Orphan Drug Designation
by the EMA and has received positive Scientific Advice from EMA that the SIERRA trial can support a marketing authorization with filing
expected in 2024.
Background on Iomab-B
Iomab-B is a first-in-class
targeted radiotherapy consisting of apamistamab, an anti-CD45 mouse antibody conjugated to radioactive iodine 131 (“I-131”)
designed to deliver targeted myeloablative radiation to malignant and hematopoietic cells prior to allogeneic BMT. CD45 is uniquely expressed
on blood cancer, immune and bone marrow stem cells at high levels. Targeting CD45 enables delivery of high radiation doses directly to
the bone marrow, with a median of 16 gray and as high as 44.6 gray in the SIERRA trial, while minimizing radiation exposure to vital organs
such as lungs, heart and gastrointestinal tract, thereby producing myeloablative outcomes with an overall better safety profile and the
tolerability of a reduced intensity regimen. I-131 is a beta- and gamma-emitting radioisotope that works on the cell surface and does
not need to be internalized. Developed at the Fred Hutchinson Cancer Research Center (“FHCRC”), Iomab-B has been studied in
multiple disease indications including leukemias, lymphomas, MDS, and MM. Over 300 patients received Iomab-B through prior studies, demonstrating
the potential for unprecedented access to BMT, improved survival and tolerability, and we intend to leverage these data as we plan for
label expansion of Iomab-B. Iomab-B has been granted Orphan Drug Designation from the FDA and has patent protection into 2037.
Actimab-A – CD33 targeting radiotherapeutic
– mutation agnostic mechanism of action has potential as combination backbone therapy in highly radiosensitive, mutation rich AML
Our Actimab-A (225Ac-lintuzumab
satetraxetan) program is focused on developing combinations with other AML treatment regimens with mechanistic synergies to establish
Actimab-A as a backbone therapy, leveraging the mutation-agnostic mechanism of action of Actimab-A. There is no known resistance mechanism
to targeted radiotherapies, making Actimab-A an attractive candidate for a variety of combinations. The scientific rationale is to use
CLAG-M, a powerful chemotherapy regimen routinely used to treat patients with r/r AML, and then use Actimab-A for its precision targeting
ability that produces double-strand-DNA breaks that lead to cancer cell death to clear out residual disease. Actimab-A has demonstrated
clinically significant survival benefit in a proof-of-concept study and is poised for advanced development in collaboration with the NCI.
Actimab-A + CLAG-M Phase 1 Study Results
In collaboration with the
Medical College of Wisconsin, the Actimab-A + CLAG-M Phase 1 trial was conducted in r/r AML patients fit for intensive therapy. These
patients had a median age of 63, failed two or more lines of therapy, which includes 57% having received prior treatment with venetoclax,
a BCL-2 inhibitor. 67% of these patients had adverse cytogenetics, 52% had a TP53 mutation, and 57% had a prior BMT. Median OS is typically
two to four months for this patient population, with a median OS of less than 3 months for patients who relapsed following venetoclax
and a median OS less than 2 months for those with a TP53 mutation.
These trial results were presented
as an oral presentation at the 2022 ASH Annual Meeting. In this difficult-to-treat r/r AML population, the results demonstrate its high
potential. We reported 1-year survival of 53% and 2-year survival of 32%, which are as much as double what can be expected with currently
available therapies. The trial showed an Overall Response Rate (“ORR”) of 65% across all dose cohorts, 52% complete remission
rate, and a 75% MRD negativity rate. As highlighted in the figure below, the results are highly encouraging and show that the high rates
of responses and MRD negativity are translating to a meaningful survival benefit in these difficult-to-treat patients, who would otherwise
have dismal outcomes.
Actimab-A + CLAG-M –Response and Survival
Benefit in r/r AML
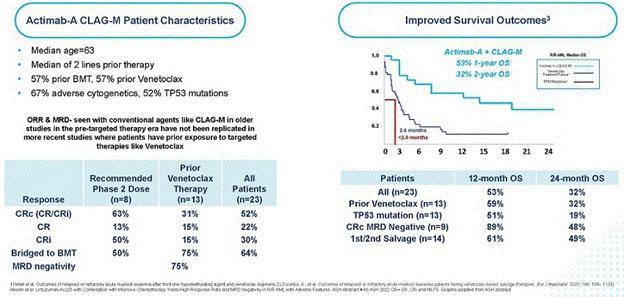
Actimab-A + CLAG-M Compared to CLAG-M Alone
in r/r AML
Efficacy of CLAG-M has been
reported in older studies (Halpern and Walter. CLAG-M with dose-escalated mitoxantrone for adults with acute myeloid leukemia. Oncotarget
2018 and Mushtaq et al. Comparison of Salvage Chemotherapy Regimens in Relapsed/Refractory Acute Myeloid Leukemia. ASH 2018) in patients
with r/r AML, however, almost all of these studies were conducted in the pre-targeted therapy era where no patients enrolled had prior
venetoclax-based therapy, thus efficacy data of CLAG-M in the current era, in patients exposed to prior venetoclax, or with other high-risk
features, is limited. When combined with Actimab-A, the combination has demonstrated a clinically significant survival benefit in a proof-of-concept
study irrespective of prior targeted treatment. R/R AML after failing venetoclax-based therapy is associated with dismal survival outcomes,
with a median OS of less than 3 months. In comparison, the combination trial of Actimab-A + CLAG-M led to 1-year survival of 59% and 2-year
survival of 32% in patients who failed prior venetoclax-based therapy, which compares very favorably to the traditional outcomes in these
patients. On September 6, 2023, updated survival data from the Actimab-A + CLAG-M combination trial was presented at SOHO with 30-month
median Overall Survival (“OS”) reported in patients with prior venetoclax treatment who proceeded to BMT and 24-month median
OS in all patients who proceeded to BMT following Actimab-A + CLAG-M treatment.
Actimab-A + venetoclax Phase 1/2 Study Results
We are conducting a Phase
1/2 multi-center trial combining Actimab-A + venetoclax in both fit and unfit patients 18 years and older with r/r AML led by UCLA Medical
Center. Data from our Actimab-A + venetoclax combination trial was presented at the 2022 ASH Annual Meeting. We have demonstrated preclinically
that combinations of Actimab-A and venetoclax have mechanistic synergies. Overexpression of MCL-1, an anti-apoptotic protein, is associated
with resistance to venetoclax in AML. Actimab-A kills tumors cells with DNA double-strand breaks and downregulates MCL-1, which can (re-)sensitize
AML cells or reduce tumor resistance to venetoclax. The Actimab-A + venetoclax combination has been well-tolerated with responses, including
a CR and a partial response in early dose escalation cohorts. In our ongoing clinical trial, we are exploring the optimal dose of Actimab-A,
as well as the dosing regimen of the combination.
Further Development for Actimab-A
In February 2023, we announced
that we entered into a CRADA with the NCI, part of the NIH, to develop Actimab-A for the treatment of patients with AML and other hematologic
malignancies. The NCI will serve as the regulatory sponsor for any clinical trials mutually approved by both parties to study Actimab-A,
and the CRADA is expected to provide extensive support for and accelerate the development of Actimab-A alone or in combination with chemotherapy,
immunotherapy, targeted agents and other novel combinations. The CRADA studies will be overseen by the NCI in collaboration with Actinium’s
clinical development team, where Actinium has the right to review and approval all protocols and has full right to all data. This broad
collaboration may accelerate our Actimab-A development efforts with access to NCI’s vast network of over 2,000 clinical trial sites
and its Myelomatch program. By year-end we expect to provide updates on our progress as we move into late-stage development with Actimab-A
+ CLAG-M, as well as other developments with our venetoclax combination trial as part of our backbone development strategy.
We are exploring the broader
opportunity with our Actimab-A program and the potential use of Actimab-A in solid tumor indications through our R&D efforts. CD33-expressing
MDSCs are present within the tumor microenvironment and exert immunosuppressive effects, and we believe that Actimab-A can play an important
role in the tumor microenvironment by depleting MDSCs in a targeted manner. In April 2023, we presented data at the AACR Annual Meeting
that we believe support the potential role of Actimab-A to overcome immunosuppression by MDSCs in the tumor microenvironment. We believe
our preclinical findings show promise with regard to Actimab-A’s ability to selectively deplete CD33-expressing MDSCs in both lung
and colorectal cancer, which we intend to explore further via clinical development. Actimab-A also demonstrated superior depletion of
human MDSCs compared to Mylotarg, a CD33-targeted ADC in colorectal cancer (p<0.01), highlighting the powerful cytotoxicity and potential
therapeutic benefit of radiotherapy compared to naked antibodies or ADCs. MDSCs are ubiquitous across multiple cancer indications and
with the substantial number of immunotherapies in development or currently in clinical use, we believe our data may support the potential
for Actimab-A, if ultimately approved for commercialization for such indication, to be a backbone therapy that could broadly improve antitumor
activity of immunotherapies such as checkpoint inhibitors and T and NK cell therapies and other therapeutic modalities in multiple solid
tumor indications. Additional preclinical data evaluating Actimab-A for the targeting of MDSCs has been accepted for presentation at the
Society of Immunotherapy of Cancer (“SITC”) 38th Annual Meeting on November 4, 2023.
Background on Actimab-A
Actimab-A is an anti-CD33
antibody linked to the potent alpha-emitting radioisotope Ac-225. Actimab-A targets CD33, which is expressed in virtually all malignant
cells in patients with AML regardless of cytogenetics or mutations and enables potent alpha radiation to be directed against radiosensitive
AML cells. These cells have no known resistance or repair mechanisms when hit with the alpha particles from the Ac-225 isotope payload
that cause double stranded DNA breaks. We believe Actimab-A is the first radiotherapeutic for r/r AML and has the unique value proposition
of broad applicability, a differentiated mechanism of action, and targeted precision that is well-tolerated with minimal toxicity. Our
CD33 development program is driven by data obtained from approximately 150 AML patients in six trials and demonstrated single agent activity
with high response rates, but was also associated with prolonged neutropenia. A combination strategy was considered appropriate given
the changing treatment landscape of AML; hence, based on presumed mechanistic synergies, an investigator-initiated trial of Actimab-A
+ CLAG-M and a company-sponsored Actimab-A + venetoclax were developed and patients were enrolled into these studies.
Conditioning Focused Programs
Iomab-B
We will further expand the
Iomab-B franchise by focusing on lifecycle management for label enhancement and indication expansion. Iomab-B data in five additional
hematologic indications (i.e., MDS, ALL, HL, NHL, and MM) provide the foundation to explore indication expansion opportunities to increase
the total addressable market for Iomab-B. Across early trials at the FHCRC, Iomab-B demonstrated similar improved access to BMT and outcomes.
We will leverage these data with strong results from the pivotal Phase 3 SIERRA trial to execute a comprehensive life cycle management
strategy to further expand Iomab-B’s role in a variety of malignant and non-malignant hematological disorders. We will continue
to develop the Iomab-B franchise to potentially address a broader market opportunity to address the over 165,000 patients diagnosed with
cancers (e.g., leukemia, lymphoma, and myeloma), who could potentially benefit from transplant, but are unable to access one today.
Iomab-ACT
Iomab-ACT is comprised of
apamistamab, the same anti-CD45 antibody as Iomab-B, but utilizes lower, nonmyeloablative levels of I-131 to achieve lymphodepletion for
cellular therapies such as CAR-T or reduced intensity conditioning for gene therapies. We intend to continue to develop the Iomab-ACT
program designed specifically for use prior to CAR-T and gene therapies, ultimately with a value proposition of improving overall access
and outcomes for patients who need cellular or gene therapies.
Preclinical data showed a
single, low-dose of Iomab-ACT demonstrated lymphodepletion and as CD45 positive immune cells are implicated in major CAR-T side effects,
i.e., cytokine release syndrome (“CRS”) and immune effector cell–associated neurotoxicity syndrome (“ICANS”),
Iomab-ACT has the potential to be developed as a conditioning agent for CAR-T therapies. CRS and ICANS remain two most common toxicities
of CAR-T therapies with severe cases (>Grade 3) seen in >20% of patients and fatality rates between 0-10%. Due to its effect on
host monocytes/macrophages, we believe conditioning with Iomab-ACT will potentially reduce the incidence of CRS and ICANS.
Unlike chemotherapy, Iomab-ACT
is targeted in nature, and we expect it to potentially promote improved CAR-T cell expansion, resulting in responses that are higher and
more durable. We believe our Iomab-ACT program is highly differentiated when compared to fludarabine and cyclophosphamide (“Flu/Cy”)
or other chemotherapy-based regimens that are used as standard practice today for lymphodepletion prior to cell therapy.
We are studying Iomab-ACT
in collaboration with MSKCC, for conditioning prior to CAR-T therapy for patients with relapsed or refractory B-cell acute lymphoblastic
leukemia (“B-ALL”) or diffuse large B-cell lymphoma (“DLBCL”). This study funded by a NIH grant is the first-of-its-kind
study to use a radiotherapeutic-based conditioning regimen with CAR-T therapy. We have completed treatment of an initial cohort of three
patients and have begun treating patients in expand to a second cohort that is being funded by our recently extended NIH grant. This study
was presented at the ASH Annual Meeting in December 2022 as a trial-in-progress. We expect to present an update on our Iomab-ACT program,
along with future development plans in the CAR-T space by year end.
R&D and Preclinical Programs
Our R&D capabilities have
the potential to yield differentiated, high-value programs that demonstrate our experience across multiple validated cancer targets and
isotopes and cover broad areas of focus leveraging our clinical development experience across hematology, targeted conditioning, solid
tumors, and next generation radiotherapies. Our programs also inform the advancement of our Iomab-B, Actimab-A, and Iomab-ACT programs.
We have utilized our technology platform to develop our clinical portfolio in hematology – Iomab-B and Actimab-A, in conditioning
for transplant and as a therapeutic, respectively. Our research collaborations with Astellas, LG Chem, and EpicentRx have established
our work with immunotherapies and in solid tumors. We are working on several preclinical programs which include novel approaches to validated
cancer targets such as HER2 and HER3, as well as novel targets that show immense potential for radiotherapeutic approaches. Underpinning
our development programs is our expanded patent portfolio of over 220 issued patents and pending patent applications worldwide.
Our platform has been used
to develop a pipeline of novel radiotherapeutic assets to drive company growth. Preclinical pharmacology studies with our targeted radiotherapeutics,
such as HER3, HER2, CD33 and CD38, have shown strong improvement in tumor growth inhibition in various preclinical tumor models as single
agents or in combination with immunotherapy such as magrolimab, an anti-CD47 monoclonal antibody. These results have prompted the team
to spearhead efforts in multiple solid tumor programs.
We continue to expand on capabilities
and technologies across therapeutic modalities, linker technologies and in vivo cancer models, and build visibility through presentations
at key conferences and publications in journals of high impact. Our R&D efforts are centered on the advancement of our key programs
with a robust “fast-to-clinic” approach in niche indications. Underpinning our development programs is our expanded patent
portfolio of over 220 issued patents and pending patent applications worldwide.
Our Platform Technology
Our proprietary technology
platform is built on the core competency to produce targeted radiotherapeutics, and coupled with our know-how and IP, establishes our
company in the development of isotope-agnostic, multi-targeted products that may address the treatment of hard-to-treat diseases. In our
clinical and preclinical programs, we have utilized multiple isotopes including Ac-225, I-131 and Lu-177 directed at multiple targets
in oncology and hematology such as CD45, CD33, CD38, HER2, among others. Our targeted radiotherapies combine the cell-killing ability
of radiation via a radioisotope payload with a targeting agent, such as a monoclonal antibody.
In addition to developing
targeted radiotherapies, we also own patents related to the manufacturing of Ac-225 in a cyclotron. We have expertise in utilizing the
alpha emitting isotope Ac-225 including clinical experience in treating approximately 150 patients with our alpha-emitter-based therapies,
“gold standard” linker technology and five issued patents in the U.S. and 49 patents internationally related to the manufacturing
or Ac-225 in a cyclotron, which we believe has the potential to produce higher quantities of highly pure Ac-225 than current methods.
When appropriate, we are well-positioned to leverage this technology to produce Ac-225.
Manufacturing
For Iomab-B, we have established
an actively managed end-to-end supply chain that encompasses isotope sourcing through drug administration at the point of care. Our end-to-end
supply chain did not miss a patient dose in our international, 24-site SIERRA Phase 3 clinical trial including 40 additional patients
that crossed over from the control arm to receive Iomab-B. We have scaled up and have commercially viable manufacturing operations in
place to support U.S. and international commercial sales.
Actinium has commercial agreements
with Contract Development and Manufacturing Organizations (“CDMOs”) with significant experience in monoclonal antibodies (“mAbs”)
and final radio-labeled drug products. The CDMO we have selected to manufacture the finished drug product to support our commercial activity
has been previously inspected by the FDA and EMA. We have scaled deliberately for manufacturing flexibility to ensure readily available
drug product upon FDA approval and the ability to ramp up rapidly to meet commercial demand.
We have multiple isotope supply
agreements and qualified vendors in place to supply isotopes for commercial production.
Intellectual Property
Our proprietary technology
platform is supported by IP, know-how and trade secrets that cover the generation, development, methods of use and manufacture of targeted
radiotherapies and their select components. Our IP covers various methods of use in multiple diseases, including indication, dose and
scheduling, radionuclide warhead, and therapeutic combinations.
As of November 2023, our patent
portfolio is comprised of over 220 issued patents and pending patent applications worldwide, which we believe constitutes a valuable business
asset. Our IP includes 47 patent families, including key patents that relate primarily to our radiotherapeutic candidates. Our patent
portfolio includes 13 issued patents and 47 pending patent applications in the U.S., and 162 that are issued or pending internationally.
The effective lives of the issued patents in our portfolio, or patents that may issue from the pending applications in our portfolio,
ranges from expirations between 2024 and 2043.
For our Iomab-B product candidate,
we have four issued patents in the U.S. and issued patents in Canada, Europe and Japan that relate to the composition. The basic patent
terms of these patents expire in 2036 and 2037. Related patent applications are also currently pending in the U.S. and internationally.
In addition, we own both U.S. and international pending patent applications that relate to the use of Iomab-B or Iomab-ACT in the treatment
of cancers and non-malignant conditions.
Our patents also cover key
areas of our business such as manufacturing key components of our product candidate, Actimab-A, including Ac-225 in a cyclotron. We have
expertise in utilizing the alpha emitting isotope Ac-225 including clinical experience in treating approximately 150 patients with our
alpha-emitter-based therapies, “gold standard” linker technology and five issued patents in the U.S. and 49 patents internationally
related to the manufacturing or Ac-225 in a cyclotron, which we believe has the potential to produce higher quantities of Ac-225 than
currently utilized methods. These patents expire in the years 2024 through 2027. In addition, we also own U.S. and international patents
and pending patent applications that relate to the manufacturing of Actimab-A and its use in the treatment of cancers.
Results of Operations –
Three Months Ended September 30, 2023 Compared to Three Months Ended September 30, 2022
The following table sets forth,
for the periods indicated, data derived from our statements of operations:
| | |
For the Three
Months Ended
September 30, | |
| (in thousands) | |
2023 | | |
2022 | |
| | |
| | |
| |
| Revenue: | |
| | |
| |
| Revenue | |
$ | - | | |
$ | - | |
| Other revenue | |
| - | | |
| 45 | |
| Total revenue | |
| - | | |
| 45 | |
| | |
| | | |
| | |
| Operating expenses: | |
| | | |
| | |
| Research and development, net of reimbursements | |
| 11,622 | | |
| 6,771 | |
| General and administrative | |
| 2,729 | | |
| 3,073 | |
| Total operating expenses | |
| 14,351 | | |
| 9,844 | |
| | |
| | | |
| | |
| Other income: | |
| | | |
| | |
| Interest income – net | |
| 1,075 | | |
| 325 | |
| Total other income | |
| 1,075 | | |
| 325 | |
| | |
| | | |
| | |
| Net loss | |
$ | (13,276 | ) | |
$ | (9,474 | ) |
Revenue
We recorded no commercial
revenue for the three months ended September 30, 2023 and September 30, 2022.
Other revenue
We determined that certain
collaborations with a third-party were within the scope of Topic ASC 606, Revenue Recognition from Contracts with Customers, or
ASC 606. The collaboration agreement were made up of multiple modules related to various research activities. While the third party had
the option to terminate the agreement at the conclusion of any module, we identified a single performance obligation to provide research
services within each module for which we received monetary consideration. The consideration is recognized to revenue over each module
and revenue of $45 thousand was recognized during the three months ended September 30, 2022. There was no corresponding revenue recognized
from a collaboration during the three months ended September 30, 2023.
On April 7, 2022, we entered
into a license and supply agreement with Immedica Pharma AB, or Immedica, pursuant to which Immedica licensed the exclusive product rights
for commercialization of Iomab-B in the European Economic Area, Middle East and North Africa (EUMENA) including Algeria, Andorra, Bahrain,
Cyprus, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Monaco, Morocco, Oman, Palestine, Qatar, San Marino, Saudi Arabia,
Switzerland, Syria, Tunisia, Turkey, the United Arab Emirates, the United Kingdom, the Vatican City and Yemen. Upon signing, we were entitled
to an upfront payment of $35 million from Immedica, which was received in May 2022. Under the terms of the License Agreement, we are eligible
to receive regulatory and commercial milestone payments and are entitled to receive royalties in the mid-20 percent range on net sales
of the product in certain countries that may result from the License Agreement. We will continue to be responsible for certain clinical
development activities and the manufacturing of Iomab-B and will retain commercialization rights in the U.S. and rest of the world.
Our contract liabilities are
recorded within Other revenue deferred – current liability or Long-term license revenue deferred in our condensed consolidated balance
sheets depending on the short-term or long-term nature of the payments to be recognized. Our contract liabilities primarily consist of
advanced payments from licensees. There was no Other revenue deferred-current liability at September 30, 2023 and December 31, 2022. Long-term
license revenue deferred was $35.0 million at September 30, 2023 and December 31, 2022, resulting from the receipt from Immedica; this
deferred revenue will be recognized upon European Union regulatory approval of Iomab-B.
Research and Development Expense, net of reimbursements
Research and development expenses
of $11.6 million for the three months ended September 30, 2023 increased $4.8 million from $6.8 million for the three months ended September
30, 2022. Higher research and development expenses were primarily due to increased CMC activity related to the planned BLA-enabling work
for Iomab-B. Once complete, CMC expenses are expected to decrease in 2024 as we expect to use final drug product material produced to
support the BLA filing and to supply initial Iomab-B commercialization. In addition, increased compensation of $1.1 million resulted due
to higher headcount necessary to support BLA-enabling CMC activity.
General and administrative expense
General and administrative
expenses of $2.7 million for the three months ended September 30, 2023 decreased by $0.4 million from $3.1 million for the three months
ended September 30, 2022. Lower professional and consulting fees of $0.5 million, lower legal fees of $0.1 million and lower non-cash
equity compensation of $0.1 million were partially offset by increased compensation of $0.3 million as a result of higher headcount.
Other income
Other income is comprised
of net interest income in both reporting periods. The amount for the three months ended September 30, 2023 of $1.1 million increased from
$0.3 million for the three months ended September 30, 2022 due to a higher average interest rate.
Net loss
Net loss of $13.3 million
for the three months ended September 30, 2023 increased by $3.8 million from $9.5 million for the three months ended September 30, 2022
primarily due to higher research and development expenses, partially offset by lower general and administrative expenses and higher other
income.
Results of Operations –
Nine months Ended September 30, 2023 Compared to Nine months Ended September 30, 2022
The following table sets forth,
for the periods indicated, data derived from our statements of operations:
| | |
For the Nine
months Ended
September 30, | |
| (in thousands) | |
2023 | | |
2022 | |
| | |
| | |
| |
| Revenue: | |
| | |
| |
| Revenue | |
$ | - | | |
$ | - | |
| Other revenue | |
| - | | |
| 1,030 | |
| Total revenue | |
| - | | |
| 1,030 | |
| | |
| | | |
| | |
| Operating expenses: | |
| | | |
| | |
| Research and development, net of reimbursements | |
| 30,552 | | |
| 15,802 | |
| General and administrative | |
| 11,025 | | |
| 8,041 | |
| Total operating expenses | |
| 41,577 | | |
| 23,843 | |
| | |
| | | |
| | |
| Other income: | |
| | | |
| | |
| Interest income – net | |
| 2,083 | | |
| 443 | |
| Total other income | |
| 2,083 | | |
| 443 | |
| | |
| | | |
| | |
| Net loss | |
$ | (39,494 | ) | |
$ | (22,370 | ) |
Revenue
We recorded no commercial
revenue for the nine months ended September 30, 2023 and September 30, 2022.
Other revenue
We determined that certain
collaborations with a third-party were within the scope of ASC 606. The collaboration agreement is made up of multiple modules related
to various research activities. While the third party has the option to terminate the agreement at the conclusion of any module, we identified
a single performance obligation to provide research services within each module for which we receive monetary consideration. Other revenue
of $0.9 million was recognized during the nine months ended September 30, 2022. There was no corresponding revenue recognized from a collaboration
during the nine months ended September 30, 2023.
The National Institutes of
Health awarded us a Small Business Technology Transfer cost reimbursable grant to support a clinical collaboration with Memorial Sloan
Kettering Cancer Center, or MSK, to study Iomab-ACT, our CD45-targeted conditioning program to achieve lymphodepletion prior to administration
of a CD19-targeted CAR T-cell therapy developed at MSK. We recognized other revenue from this grant for the nine months ended September
30, 2022 of $0.1 million. There was no other revenue recognized for the nine months ended September 30, 2023.
Research and Development Expense, net of reimbursements
Research and development expenses
of $30.6 million for the nine months ended September 30, 2023 increased $14.8 million from $15.8 million for the nine months ended September
30, 2022. Higher research and development expenses were primarily due to increased CMC activity related to the planned BLA-enabling work
for Iomab-B, which once complete, we expect to decrease in 2024 as we expect to use final drug product material produced to support the
BLA filing and to supply initial Iomab-B commercialization. In addition, increased compensation of $3.2 million resulted due to higher
headcount primarily to support BLA-enabling CMC activity.
General and administrative expense
General and administrative
expenses of $11.0 million for the nine months ended September 30, 2023 increased by $3.0 million from $8.0 million for the nine months
ended September 30, 2022. Higher expenses were primarily due to increased compensation of $1.1 million due to higher headcount, higher
non-cash equity compensation of $0.8 million, and higher professional and consulting fees, including recruiting fees.
Other income
Other income is comprised
of net interest income in both reporting periods. The amount for the nine months ended September 30, 2023 of $2.1 million increased from
$0.4 million for the nine months ended September 30, 2022 due to a higher average interest rate.
Net loss
Net loss of $39.5 million
for the nine months ended September 30, 2023 increased by $17.1 million from $22.4 million for the nine months ended September 30, 2022
primarily due to higher research and development expenses and general and administrative expenses.
Liquidity and Capital Resources
The following table sets forth
selected cash flow information for the periods indicated:
| |
|
For the Nine months Ended
September 30, |
|
| (in thousands) |
|
2023 |
|
|
2022 |
|
| |
|
|
|
|
|
|
| Cash (used in)/provided by operating activities |
|
$ |
(39,845 |
) |
|
$ |
16,422 |
|
| Cash used in investing activities |
|
|
(153 |
) |
|
|
(350 |
) |
| Cash provided by financing activities |
|
|
13,678 |
|
|
|
18,216 |
|
| |
|
|
|
|
|
|
|
|
| Net change in cash, cash equivalents and restricted cash |
|
$ |
(26,320 |
) |
|
$ |
34,288 |
|
Net cash used in operating
activities for the nine months ended September 30, 2023 of $39.8 million increased by $56.2 million from the prior-year period of $16.4
million provided by operating activities, as a result of the higher net loss of $17.1 million and the receipt of the $35.0 million up-front
payment from Immedica included in the prior-year period.
Net cash used in investing
activities was $0.1 million and $0.4 million for the nine months ended September 30, 2023 and 2022, respectively, due to the purchase
of equipment.
Net cash provided by financing
activities for the nine months ended September 30, 2023 of $13.7 million and for the nine months ended September 30, 2022 of $18.2 million
was primarily from the sale of shares of our common stock.
In August 2020 we entered
into the Capital on Demand™ Sales Agreement with JonesTrading Institutional Services LLC, or JonesTrading, pursuant to which we
may sell, from time to time, through or to JonesTrading, up to an aggregate of $200 million of our common stock. On June 28, 2022, we
entered into an Amended and Restated Capital on Demand™ Sales Agreement, or the Amended Sales Agreement, with JonesTrading and B.
Riley Securities, Inc. The Amended Sales Agreement modifies the original Capital on Demand™ Sales Agreement to include B. Riley
as an additional sales agent thereunder. Shares of common stock are offered pursuant to our shelf registration statement on Form S-3 filed
with the SEC on August 7, 2020. For the nine months ended September 30, 2023, we sold 1.7 million shares of common stock, resulting in
gross proceeds of $13.8 million and net proceeds of $13.4 million. For the nine months ended September 30, 2022, we sold 3.0 million shares
of common stock, resulting in gross proceeds of $18.9 million and net proceeds of $18.3 million.
As of the date of filing this
report, we expect that our existing resources will be sufficient to fund our planned operations for more than 12 months following the
date of this report.
Critical Accounting Policies and Use of Estimates
Our management’s discussion
and analysis of financial condition and results of operations is based on our consolidated financial statements, which have been prepared
in accordance with accounting principles generally accepted in the United States, (“GAAP”). The preparation of these financial
statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities and expenses and the disclosure
of contingent assets and liabilities in our consolidated financial statements during the reporting periods. These items are monitored
and analyzed by us for changes in facts and circumstances, and material changes in these estimates could occur in the future. We base
our estimates on historical experience, known trends and events, and on various other factors that we believe are reasonable under the
circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not
readily apparent from other sources. Changes in estimates are reflected in reported results for the period in which they become known.
Actual results may differ materially from these estimates under different assumptions or conditions.
Our significant accounting
policies are described in detail in the notes to our consolidated financial statements appearing in our Annual Report filed on Form 10-K
for the year ended December 31, 2022.
Fair Value Measurement
Fair value is defined as the
price that would be received to sell an asset, or paid to transfer a liability, in an orderly transaction between market participants.
A fair value hierarchy has been established for valuation inputs that gives the highest priority to quoted prices in active markets for
identical assets or liabilities and the lowest priority to unobservable inputs.
Revenue Recognition
We recognize revenue in accordance
with ASC 606. Under ASC 606, we recognize revenue when our customer obtains control of promised goods or services, in an amount that reflects
the consideration that we expect to receive in exchange for those goods or services. To determine revenue recognition for arrangements
within the scope of ASC 606, we perform the following five steps: (i) identify the contract(s) with a customer; (ii) identify the performance
obligations in the contract; (iii) determine the transaction price, including variable consideration, if any; (iv) allocate the transaction
price to the performance obligations in the contract; and (v) recognize revenue as we satisfy a performance obligation. We only apply
the five-step model to contracts when it is probable that we will collect the consideration to which we are entitled in exchange for the
goods or services we transfer to the customer.
At contract inception, once
the contract is determined to be within the scope of ASC 606, we assess whether the promised goods or services promised within each contract
are distinct and, therefore, represent a separate performance obligation. Goods and services that are determined not to be distinct
are combined with other promised goods and services until a distinct bundle is identified. In determining whether goods or services are
distinct, we evaluate certain criteria, including whether (i) the customer can benefit from the good or service either on its own
or together with other resources that are readily available to the customer (capable of being distinct) and (ii) the good or service
is separately identifiable from other goods or services in the contract (distinct in the context of the contract).
ASC 606 requires us to allocate
the arrangement consideration on a relative standalone selling price basis for each performance obligation after determining the transaction
price of the contract and identifying the performance obligations to which that amount should be allocated. The relative standalone selling
price is defined in the new revenue standard as the price at which an entity would sell a promised good or service separately to a customer.
We then recognize as revenue the amount of the transaction price that is allocated to the respective performance obligation as each performance
obligation is satisfied, either at a point in time or over time, and if over time, recognition is based on the use of an output or input
method.
Collaborative Arrangements
We follow the accounting guidance
for collaboration agreements, which requires that certain transactions between us and collaborators be recorded in our consolidated statements
of operations on either a gross basis or net basis, depending on the characteristics of the collaborative relationship, and requires enhanced
disclosure of collaborative relationships. We evaluate our collaboration agreements for proper classification in our consolidated statements
of operations based on the nature of the underlying activity. When we conclude that we have a customer relationship with one of our collaborators,
we follow the guidance of ASC 606.
Grant Revenue
We had a grant from a government-sponsored
entity for research and development related activities that provided for payments for reimbursed costs, which included overhead and general
and administrative costs as well as an administrative fee. We recognized revenue from the grant as we performed services under this arrangement.
Associated expenses were recognized when incurred as research and development expense. Revenue and related expenses are presented gross
in the consolidated statements of operations.
License Revenue
We entered into a product
licensing agreement whereby we allowed a third party to commercialize a certain product in specified territories using our trademarks.
The terms of this arrangement includes payment to us for a combination of one or more of the following: upfront license fees; development,
regulatory and sales-based milestone payments; and royalties on net sales of licensed products. We use judgment to determine whether milestones
or other variable consideration should be included in the transaction price.
Upfront license fees:
If the license to our intellectual property is determined to be distinct from the other performance obligations identified in the arrangement,
we will recognize revenue from upfront license fees allocated to the license when the license is transferred to the licensee and the licensee
is able to use and benefit from the license. For licenses that are bundled with other promises, we determine whether the combined performance
obligation is satisfied over time or at a point in time.
Development, regulatory
or commercial milestone payments: At the inception of each arrangement that includes payments based on the achievement of certain
development, regulatory and sales-based or commercial events, we evaluate whether the milestones are considered probable of being achieved
and estimate the amount to be included in the transaction price using the most likely amount method. If it is probable that a significant
revenue reversal would not occur, the associated milestone value is included in the transaction price. Milestone payments that are not
within our or the licensee’s control, such as regulatory approvals, are not considered probable of being achieved until regulatory
approval is received. At the end of each subsequent reporting period, we will re-evaluate the probability of achieving such development
and regulatory milestones and any related constraint, and if necessary, adjust our estimate of the overall transaction price. Any such
adjustments are recorded on a cumulative catch-up basis and recorded as part of license revenues during the period of adjustment.
Sales-based milestone payments
and royalties: For arrangements that include sales-based royalties, including milestone payments based on the volume of sales, we
will determine whether the license is deemed to be the predominant item to which the royalties or sales-based milestones relate and if
such is the case, we will recognize revenue at the later of (i) when the related sales occur, or (ii) when the performance obligation
to which some or all of the royalty has been allocated has been satisfied (or partially satisfied).
Upfront payments and fees
may require deferral of revenue recognition to a future period until we perform our obligations under these arrangements or when it is
probable that a significant reversal in the amount of cumulative revenue recognized will not occur when the uncertainty associated with
any variable consideration is subsequently resolved. Amounts payable to us are recorded as accounts receivable when our right to consideration
is unconditional.
Research and Development Costs
Research and development costs
are expensed as incurred. These costs include the costs of manufacturing drug components and final drug product, the costs of clinical
trials, costs of employees and associated overhead, and depreciation and amortization costs related to facilities and equipment. Research
and development reimbursements are recorded by us as a reduction of research and development costs.
Share-Based Payments
We estimate the fair value
of each stock option award at the grant date by using the Black-Scholes option pricing model. The fair value determined represents the
cost for the award and is recognized over the vesting period during which an employee is required to provide service in exchange for the
award. We account for forfeitures of stock options as they occur.
Accounting Standards Recently Adopted
In November 2021, the FASB
issued ASU 2021-10, Government Assistance (Topic 832), Disclosures by Business Entities about Government Assistance, which provides
guidance on disclosure requirements to entities other than not-for-profit entities about transaction with a government that are accounted
for by applying a grant or contribution accounting model by analogy. ASU 2021-10 requires an entity to make annual disclosures related
to (1) the nature of the transactions and the related accounting policy used to account for the government transactions, (2) quantification
and disclosure of amounts related to the government transactions included in balance sheet and income statement financial statement line
items, and (3) significant terms and conditions of the government transactions, including commitments and contingencies. The amendments
of ASU 2021-10 are effective January 1, 2022, including interim periods. We adopted this standard effective January 1, 2022 and the standard
did not have a material impact on our financial statements.
In October 2021, FASB issued
ASU 2021-08, Business Combinations (Topic 805), Account for Contract Assets and Contract Liabilities from Contracts with Customers,
which provides guidance on accounting for contract assets and contract liabilities acquired in a business combination in accordance ASC
606. To achieve this, an acquirer may assess how the acquiree applied ASC 606 to determine what to record for the acquired revenue contracts.
Generally, this should result in an acquirer recognizing and measuring the acquired contract assets and contract liabilities consistent
with how they were recognized and measured in the acquiree’s financial statements. The amendments of ASU 2021-08 are effective January
1, 2023, including interim periods. We will evaluate the impact of ASU 2021-08 on any future business combinations that we may enter in
the future.
In May 2021, the Financial
Accounting Standards Board, or FASB, issued ASU 2021-04, Earnings Per Share (topic 260), Debt — Modifications and Extinguishments
(Subtopic 470-50), Compensation – Stock Compensation (Topic 718) and Derivatives and Hedging – Contracts in an Entity’s
Own Equity (Subtopic 815-40) – Issuer’s Accounting for Certain Modifications or Exchanges of Freestanding Equity-Classified
Written Call Options, which provides guidance of a modification or an exchange of a freestanding equity-classified written call option
that remains equity classified after modification or exchange as (1) an adjustment to equity and, if so, the related earnings per share
(EPS) effects, if any, or (2) an expense and, if so, the manner and pattern of recognition. The amendments in this ASU are effective January
1, 2022, including interim periods. We adopted this standard effective January 1, 2022 and the standard did not have a material effect
on our financial statements.
ITEM 3. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET
RISK.
We are not currently exposed
to significant market risk related to changes in interest rates. As of September 30, 2023, our cash equivalents consisted primarily of
short-term money market funds. Our primary exposure to market risk is interest rate sensitivity, which is affected by changes in the general
level of U.S. interest rates. Due to the short-term nature of the cash equivalents in our portfolio and the low risk profile of our cash
equivalents, an immediate 10% change in interest rates would not have a material effect on the fair market value of our financial position
or results of operations.
We are not currently exposed
to significant market risk related to changes in foreign currency exchange rates. Our operations may be subject to fluctuations in foreign
currency exchange rates in the future.
Inflation generally affects
us by increasing our cost of labor and clinical trial costs. We do not believe that inflation had a material effect on our business, financial
condition or results of operations during the nine months ended September 30, 2023 and 2022.
ITEM 4. CONTROLS AND PROCEDURES.
Evaluation of Disclosure
Controls and Procedures. Under the supervision and with the participation of our management, including our principal executive
officer and principal financial and accounting officer, we conducted an evaluation of the effectiveness, as of September 30, 2023, of
our disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended,
or the Exchange Act. Based upon such evaluation, our principal executive officer and principal financial and accounting officer have concluded
that, as of September 30, 2023, our disclosure controls and procedures were effective to provide reasonable assurance that the information
we are required to disclose in our filings with the Securities and Exchange Commission, or SEC, under the Exchange Act (i) is recorded,
processed, summarized and reported within the time periods specified in the SEC’s rules and forms and (ii) accumulated and communicated
to our management, including our principal executive officer and principal financial and accounting officer, as appropriate to allow timely
decisions regarding required disclosure.
Changes in Internal Control
over Financial Reporting. There were no changes in our system of internal controls over financial reporting during the period covered
by this report that has materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
PART II – OTHER INFORMATION
ITEM 1. LEGAL PROCEEDINGS
None.
ITEM 1A. RISK FACTORS
In analyzing our company,
you should consider carefully the following risk factors, together with all of the other information included in this Quarterly Report
on Form 10-Q. Factors that could cause or contribute to differences in our actual results include those discussed in the following
subsection, as well as those discussed above in “Management’s Discussion and Analysis of Financial Condition and Results of
Operations” and in our Annual Report filed on Form 10-K for the year ended December 31, 2022. Each of the following risk factors,
either alone or taken together, could adversely affect our business, operating results and financial condition, as well as adversely affect
the value of an investment in our company. The risks and uncertainties described below are not the only ones we face. Additional risks
not currently known to us or other factors not perceived by us to present significant risks to our business at this time also may impair
our business operations.
Summary of Risk Factors
We are providing the following
summary of the risk factors contained in this Report on Form 10-Q to enhance the readability and accessibility of our risk factor disclosures.
We encourage you to carefully review the full risk factors contained in our Annual Report on Form 10-K for the year ended December 31,
2022 in their entirety for additional information regarding the material factors that make an investment in our securities speculative
or risky. These risks and uncertainties include, but are not limited to, the following:
| |
● |
We are a clinical-stage company and have generated no revenue from commercial sales to date; |
| |
|
|
| |
● |
We have incurred net losses in every year since our inception and anticipate that we will continue to incur net losses in the future; |
| |
|
|
| |
● |
If we fail to obtain additional financing, we will be unable to continue or complete our product development or product commercialization and you will likely lose your entire investment; |
| |
|
|
| |
● |
We are highly dependent on the regulatory and commercial success of Iomab-B |
| |
|
|
| |
● |
Our business could be adversely affected by the effects of health epidemics, including the global COVID-19 pandemic; |
| |
|
|
| |
● |
We have not demonstrated that any of our products are safe and effective for any indication and will continue to expend substantial time and resources on clinical development before any of our current or future product candidates will be eligible for FDA approval, if ever; |
| |
|
|
| |
● |
Our clinical trials may fail to demonstrate adequately the efficacy and safety of our product candidates, which would prevent or delay regulatory approval and commercialization; |
| |
|
|
| |
● |
Preliminary, Interim, and “top-line” data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject to audit and verification procedures that could result in material changes in the final data.; |
| |
|
|
| |
● |
Healthcare legislative reform measures intended to increase pressure to reduce prices of pharmaceutical products paid for by Medicare or, otherwise, affect the federal regulation of the U.S. healthcare system could have a material adverse effect our business, future revenue, if any, and results of operations; |
| |
● |
We rely on third parties to conduct our clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines or comply with regulatory requirements, we may not be able to obtain regulatory approval for or commercialize our product candidates; |
| |
|
|
| |
● |
We currently depend on single third-party manufacturers to produce our pre-clinical and clinical trial drug supplies. Any disruption in the operations of our current third-party manufacturers, or other third-party manufacturers we may engage in the future, could adversely affect our business and results of operations; |
| |
● |
Our product candidates may cause undesirable side effects or have other properties that could halt their clinical development, prevent their regulatory approval, limit their commercial potential, or result in significant negative consequences; |
| |
|
|
| |
● |
Our patent position is highly uncertain and involves complex legal and factual questions. |
| |
|
|
| |
● |
The use of hazardous materials, including radioactive and biological materials, in our research and development efforts imposes certain compliance costs on us and may subject us to liability for claims arising from the use or misuse of these materials; |
| |
|
|
| |
● |
We are highly dependent on our key personnel, and the demand for talent in the biotechnology industry is highly competitive; if we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement or execute our business strategy; |
| |
|
|
| |
● |
Certain provisions of our Certificate of Incorporation and Bylaws and Delaware law make it more difficult for a third party to acquire us and make a takeover more difficult to complete, even if such a transaction were in our stockholders’ interest; and |
| |
|
|
| |
● |
Our ability to utilize our net operating loss carryforwards and certain other tax attributes may be limited. |
Risks Related to Our Business
We are a clinical-stage company and have
generated no revenue from commercial sales to date.
We are a clinical-stage biopharmaceutical
company with a limited operating history. We have no products approved for commercial sale and have not generated any revenue from product
sales to date. We will encounter risks and difficulties frequently experienced by early-stage companies in rapidly evolving fields. If
we do not address these risks successfully, our business will suffer.
We have incurred net losses in every year
since our inception and anticipate that we will continue to incur net losses in the future.
We are not profitable and
have incurred losses in each period since our inception. As of September 30, 2023 and December 31, 2022, we had an accumulated deficit
of $328.3 million and $288.8 million, respectively. We reported a net loss of $39.5 million and $22.4 million for the nine months ended
September 30, 2023 and 2022, respectively. We expect to continue to operate at a net loss as we continue our research and development
efforts, continue to conduct clinical trials and develop manufacturing, sales, marketing and distribution capabilities. There can be no
assurance that the products under development by us will be approved for sale in the United States or elsewhere. Furthermore, there can
be no assurance that if such products are approved, they will be successfully commercialized, which would have an adverse effect on our
business prospects, financial condition and results of operation.
If we fail to obtain additional financing,
we will be unable to continue or complete our product development and you will likely lose your entire investment.
As of the date of filing this
report, we expect that our existing resources will be sufficient to fund our planned operations for more than 12 months following the
date of this report.
Our business or operations
may change in a manner that would consume available funds more rapidly than anticipated and substantial additional funding may be required
to maintain operations, fund expansion, develop new or enhanced products, acquire complementary products, business or technologies or
otherwise respond to competitive pressures and opportunities, such as a change in the regulatory environment or a change in preferred
cancer treatment modalities. However, we may not be able to secure funding when we need it or on favorable terms or indeed on any terms.
In addition, from time to time, we may not be able to secure enough capital in a timely enough manner which may cause the generation of
a going-concern opinion from our auditors which can and may impair our stock market valuation and also our ability to finance on favorable
terms or indeed on any terms.
To raise additional capital,
we may in the future offer additional shares of our common stock or other securities convertible into or exchangeable for our common stock.
We cannot assure you that we will be able to sell shares or other securities in any other offering at a price per share that is equal
to or greater than the price per share paid by investors, and investors purchasing shares or other securities in the future could have
rights superior to existing stockholders.
If we cannot raise adequate
funds to satisfy our capital requirements, we will have to delay, scale back or eliminate our research and development activities, clinical
studies or future operations. We may also be required to obtain funds through arrangements with collaborators, which arrangements may
require us to relinquish rights to certain technologies or products that we otherwise would not consider relinquishing, including rights
to future product candidates or certain major geographic markets. We may further have to license our technology to others. This could
result in sharing revenues which we might otherwise have retained for ourselves. Any of these actions may harm our business, financial
condition and results of operations.
The amount of funding we will
need depends on many factors, including the progress, timing and scope of our product development programs; the progress, timing and scope
of our preclinical studies and clinical trials; the time and cost necessary to obtain regulatory approvals; the time and cost necessary
to further develop manufacturing processes and arrange for contract manufacturing; our ability to enter into and maintain collaborative,
licensing and other commercial relationships; and our partners’ commitment of time and resources to the development and commercialization
of our products.
We have limited access to the capital markets
and even if we can raise additional funding, we may be required to do so on unfavorable terms.
We have limited access to
the capital markets to raise funds. The capital markets have been unpredictable in the recent past for radioisotope and other oncology
companies and unprofitable companies such as ours. In addition, it is generally difficult for development-stage companies to raise capital
under current market conditions. The amount of capital that a company such as ours is able to raise often depends on variables that are
beyond our control. As a result, we may not be able to secure financing on terms attractive to us, or at all. If we are able to consummate
a financing arrangement, the amount raised may not be sufficient to meet our future needs. If adequate funds are not available on acceptable
terms, or at all, our business, including our technology licenses, results of operations, financial condition and our continued viability
will be materially adversely affected.
We are highly dependent on the regulatory
and commercial success of Iomab-B
We have completed patient
enrollment in the pivotal Phase 3 SIERRA trial (Study of Iomab-B in Elderly Relapsed or Refractory AML), a 153-patient multi-center randomized
trial that compared outcomes of patients who receive Iomab-B and a BMT to those of patients receiving physician’s choice of salvage
chemotherapy, defined as conventional care, as no standard of care exists for this patient population. We have announced that Iomab-B
met the primary endpoint of dCR in the SIERRA trial with statistical significance (p<0.0001) and we intend to submit a BLA with the
FDA in 2024. Even if Iomab-B receives favorable regulatory approval, we may not be successful in securing adequate reimbursement or establishing
successful commercial operations. Any or all of these factors could have a material adverse impact on our business and ability to continue
operations.
We may be unable to establish sales, marketing
and commercial supply capabilities.
We do not currently have,
nor have we ever had, commercial sales and marketing capabilities. If any of our product candidates become approved, we would have to
build and establish these capabilities in order to commercialize our approved product candidates. The process of establishing commercial
capabilities will be expensive and time consuming. Even if we are successful in building sales and marketing capabilities, we may not
be successful in commercializing any of our product candidates. Any delays in commercialization or failure to successfully commercialize
any product candidate may have material adverse impacts on our business and ability to continue operations.
Our business could be adversely affected
by the effects of health epidemics, including the global COVID-19 pandemic.
The global health crisis caused
by the novel coronavirus COVID-19 pandemic and its resurgences has had and may in the future negatively impact global economic activity.
Although the Public Health Emergency for COVID-19 declared by the U.S. federal government has ended, there remains a risk that new variants
of COVID 19, or other infectious diseases, may still emerge. The full impact of such an event cannot be predicted at this time, and could
depend on numerous factors, including vaccination rates among the population, the effectiveness of COVID-19 vaccines and boosters against
the COVID-19 variants and the response by governmental bodies and regulators. Given the ongoing and dynamic nature of the circumstances,
it is difficult to predict the impact of a future pandemic on our business.
Many countries around the
world imposed quarantines and restrictions on travel and mass gatherings in response to the COVID-19 pandemic and could reinstitute such
policies in response to future infectious disease outbreaks. In such a scenario, our ability to continue to operate our business may
also be limited. Such events may result in a period of business, supply and drug product manufacturing disruption, and in reduced operations,
any of which could materially affect our business, financial condition and results of operations. New outbreaks may further divert the
attention and efforts of the medical community to coping with such outbreaks and may disrupt the marketplace in which we operate and
may have a material adverse effect on our operations.
Market disruption and volatility
following a new outbreak of infectious disease could have an adverse effect on our ability to access capital, which could in turn negatively
affect our liquidity. In addition, a recession or market correction resulting from the spread of such disease could materially affect
our business and the value of our common stock.
A future pandemic could adversely
affect our clinical trial operations, including our ability to conduct the trials on the expected timelines and recruit and retain patients
and principal investigators and site staff who, as healthcare providers, may have heightened exposure to a future pandemic if their geography
is impacted by the pandemic. Further, future pandemic could result in delays in our clinical trials due to prioritization of hospital
resources toward the pandemic, restrictions in travel, potential unwillingness of patients to enroll in trials at this time, or the inability
of patients to comply with clinical trial protocols if quarantines or travel restrictions are reinstated that impede patient movement
or interrupt healthcare services. In addition, we rely on independent clinical investigators, contract research organizations and other
third-party service providers to assist us in managing, monitoring and otherwise carrying out our preclinical studies and clinical trials,
and the pandemic may affect their ability to devote sufficient time and resources to our programs or to travel to sites to perform work
for us, which may result in delays or hinder our ability to collect data from our clinical trials.
Additionally, a future pandemic
may result in delays in receiving approvals from local and foreign regulatory authorities, delays in necessary interactions with IRB’s
or Institutional Review Boards, local and foreign regulators, ethics committees and other important agencies and contractors due to limitations
in employee resources or forced furlough of government employees.
Our business is subject to cybersecurity
risks.
Our operations are increasingly
dependent on information technologies and services. Threats to information technology systems associated with cybersecurity risks and
cyber incidents or attacks continue to grow, and include, among other things, storms and natural disasters, terrorist attacks, utility
outages, theft, viruses, phishing, malware, design defects, human error, and complications encountered as existing systems are maintained,
repaired, replaced, or upgraded. Risks associated with these threats include, among other things:
| |
● |
theft or misappropriation of funds; |
| |
|
|
| |
● |
loss, corruption, or misappropriation of intellectual property, or other proprietary, confidential or personally identifiable information (including supplier, clinical data or employee data); |
| |
|
|
| |
● |
disruption or impairment of our and our business operations and safety procedures; |
| |
|
|
| |
● |
damage to our reputation with our potential partners, patients and the market; |
| |
|
|
| |
● |
exposure to litigation; |
| |
|
|
| |
● |
increased costs to prevent, respond to or mitigate cybersecurity events. |
Although we utilize various
procedures and controls to mitigate our exposure to such risk, cybersecurity attacks and other cyber events are evolving and unpredictable.
Moreover, we have no control over the information technology systems of third parties conducting our clinical trials, our suppliers, and
others with which our systems may connect and communicate. As a result, the occurrence of a cyber incident could go unnoticed for a period
time.
We have cybersecurity insurance
coverage in the event we become subject to various cybersecurity attacks, however, we cannot ensure that it will be sufficient to cover
any particular losses we may experience as a result of such cyberattacks. Any cyber incident could have a material adverse effect on our
business, financial condition and results of operations.
Risks Related to Regulation
The FDA or comparable foreign regulatory
authorities may disagree with our regulatory plans and we may fail to obtain regulatory approval of our product candidates.
Our products are subject to
rigorous regulation by the FDA and numerous other federal, state and foreign governmental authorities. The process of seeking regulatory
approval to market an antibody radiation-conjugate product is expensive and time-consuming, and, notwithstanding the effort and expense
incurred, approval is never guaranteed. If we are not successful in obtaining timely approval of our products from the FDA, we may never
be able to generate significant revenue and may be forced to cease operations. In particular, the FDA permits commercial distribution
of a new antibody radiation-conjugate product only after a BLA for the product has received FDA approval. The BLA process is costly, lengthy
and inherently uncertain. Any BLA filed by us will have to be supported by extensive data, including, but not limited to, technical, preclinical,
clinical trial, chemistry, manufacturing and controls (“CMC”) and labeling data, to demonstrate to the FDA’s satisfaction
the safety and efficacy of the product for its intended use. The lengthy approval process as well as the unpredictability of future clinical
trial results may result in our failing to obtain regulatory approval to market our product candidates, which would significantly harm
our business, results of operations and prospects. In addition, even if we were to obtain approval, regulatory authorities may approve
any of our product candidates for fewer or more limited indications than we request, may not approve the price we intend to charge for
our products, may grant approval contingent on the performance of costly post-marketing clinical trials, or may approve a product candidate
with a label that does not include the labeling claims necessary or desirable for the successful commercialization of that product candidate.
Any of the foregoing scenarios could materially harm the commercial prospects for our product candidates.
In June 2012, we acquired
rights to apamistamab, a clinical stage anti-CD45 monoclonal antibody with safety and efficacy data in more than 300 patients in need
of a BMT. Iomab-B is our product candidate that links I-131 to apamistamab that was studied in the pivotal Phase 3 SIERRA trial. Product
candidates utilizing apamistamab would require BLA approval before they can be marketed in the United States. We are also evaluating Iomab-ACT,
which uses a lower dose I-131 for lymphodepletion prior to CAR-T or adoptive cell therapy. We are currently evaluating clinical trials
that would use our construct for lymphodepletion. Our CD33 Alpha program studying Actimab-A (lintuzumab-Ac-225) product candidate is also
being studied in several Phase 1 trials under our sponsorship and investigator-initiated trials in patients with r/r AML. Product candidates
utilizing the lintuzumab antibody would require BLA approval before they can be marketed in the United States. We are in the early stages
of evaluating other product candidates consisting of conjugates of Ac-225 with human or humanized antibodies for pre-clinical and clinical
development in other types of cancer. The FDA may not approve these products for the indications that are necessary or desirable for successful
commercialization. The FDA may fail to approve any BLA we submit for new product candidates or for new intended uses or indications for
approved products or future product candidates. Failure to obtain FDA approval for our products in the proposed indications would have
a material adverse effect on our business prospects, financial condition and results of operations.
The approval process in the
United States and in other countries could result in unexpected and significant costs for us and consume management’s time and other
resources. The FDA and other foreign regulatory agencies could ask us to supplement our submissions, collect non-clinical data, conduct
additional clinical trials or engage in other time-consuming actions, or it could simply deny our applications. In addition, even if we
obtain approval to market our products in the United States or in other countries, the approval could be revoked, or other restrictions
imposed if post-market data demonstrates safety issues or lack of effectiveness. We cannot predict with certainty how, or when, the FDA
or other regulatory authorities will act. If we are unable to obtain the necessary regulatory approvals, our financial condition and cash
flow may be materially adversely affected, and our ability to grow domestically and internationally may be limited. Additionally, even
if we obtain approval, regulatory authorities may approve any of our product candidates for fewer or more limited indications that we
request. The Company’s products may not be approved for the specific indications that are most necessary or desirable for successful
commercialization or profitability.
We have not demonstrated that any of our
products are safe and effective for any indication and will continue to expend substantial time and resources on clinical development
before any of our current or future product candidates will be eligible for FDA approval, if ever.
We expect that a substantial
portion of our efforts and expenditures over the next few years will be devoted to development of our existing and contemplated biological
product candidates. Accordingly, our business currently depends heavily on the successful development, FDA approval, and commercialization
of such candidates, which may never receive FDA approval or be successfully commercialized even if FDA approval is received. The research,
testing, manufacturing, labeling, approval, sale, marketing, and distribution of our biological product candidates are, and will remain,
subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, as applicable. We
are currently not permitted to market any of our current or future product candidates in the United States until we receive FDA approval
(of each) via the BLA process. To date, we have two product candidates in clinical development and have not-yet submitted a BLA for any
of our candidates and, for many such candidates, do not expect to be in a position to do so for the foreseeable future, as there are numerous
developmental steps that must be completed before we can prepare and submit a BLA.
In the United States, the FDA regulates pharmaceutical
and biological product candidates under the FDCA and the Public Health Service Act (“PHSA”), as well as their respective
implementing regulations. Such products and product candidates are also subject to other federal, state, and local statutes and regulations.
The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local, and foreign statutes
and regulations requires the expenditure of substantial time and financial resources. The process required by the FDA before a drug or
biological product may be marketed in the United States generally involves the following:
| |
● |
completion of preclinical laboratory tests and animal studies in accordance with FDA’s good laboratory practices (“GLPs”) and applicable requirements for the humane use of laboratory animals or other applicable regulations; |
| |
● |
submission to the FDA of an Investigational New Drug (“IND”), which must become effective before human clinical trials in the United States may begin; |
| |
● |
performance of adequate and well-controlled human clinical trials in accordance with FDA’s IND regulations, GCPs, and any additional requirements for the protection of human research subjects and their health information, to establish the safety and efficacy of the proposed biological product for its intended use; |
| |
|
|
| |
● |
submission to the FDA of a BLA for marketing approval that meets applicable requirements to ensure the continued safety, purity, and potency of the product that is the subject of the BLA based on results of preclinical testing and clinical trials; |
| |
|
|
| |
● |
satisfactory completion of an FDA inspection of the manufacturing facility or facilities where the biological product is produced, to assess compliance with cGMPs and assure that the facilities, methods and controls are adequate to preserve the biological product’s identity, strength, quality and purity; |
| |
|
|
| |
● |
potential FDA audit of the nonclinical study and clinical trial sites that generated the data in support of the BLA; and |
| |
|
|
| |
● |
FDA review and approval, or denial, of the BLA. |
Before testing any biological
product candidate in humans, the product candidate enters the preclinical testing stage. Preclinical tests include laboratory evaluations
of product chemistry, toxicity and formulation, as well as animal studies to assess the potential safety and activity of the product candidate.
The conduct of the preclinical tests must comply with federal regulations and requirements including GLPs. The clinical trial sponsor
must submit the results of the preclinical tests, together with manufacturing information, analytical data, any available clinical data
or literature and a proposed clinical protocol, to the FDA as part of the IND. Some preclinical testing may continue even after the IND
is submitted. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA raises concerns or questions regarding
the proposed clinical trials and places the trial on a clinical hold within that 30-day time period. In such a case, the IND sponsor and
the FDA must resolve any outstanding concerns before the clinical trial can begin. The FDA may also impose clinical holds on a biological
product candidate at any time before or during clinical trials due to safety concerns or non-compliance. If the FDA imposes a clinical
hold, trials may not recommence without FDA authorization and then only under terms authorized by the FDA. Accordingly, we cannot be sure
that submission of an IND will result in the FDA allowing clinical trials to begin or that, for those that have already commenced under
an active IND, that issues will not arise that suspend or terminate such trials.
Clinical trials involve the
administration of the biological product candidate to healthy volunteers or patients under the supervision of qualified investigators,
generally physicians not employed by or under the trial sponsor’s control. Clinical trials are conducted under protocols detailing,
among other things, the objectives of the clinical trial, dosing procedures, subject selection and exclusion criteria, and the parameters
to be used to monitor subject safety, including stopping rules that assure a clinical trial will be stopped if certain adverse events
should occur. Each protocol and any amendments to the protocol must be submitted to the FDA as part of the IND. Clinical trials must
be conducted and monitored in accordance with the FDA’s regulations composing the GCP requirements, including the requirement that
all research subjects provide informed consent. Further, each clinical trial must be reviewed and approved by an independent institutional
review board, or IRB, at or servicing each institution at which the clinical trial will be conducted. An IRB is charged with protecting
the welfare and rights of trial participants and considers such items as whether the risks to individuals participating in the clinical
trials are minimized and are reasonable in relation to anticipated benefits. The IRB also approves the form and content of the informed
consent that must be signed by each clinical trial subject or his or her legal representative and must monitor the clinical trial until
completed. Human clinical trials are typically conducted in three sequential phases that may overlap or be combined:
| |
● |
Phase 1. The biological product is initially introduced into healthy human subjects and tested for safety. In the case of some products for severe or life-threatening diseases, especially when the product may be too inherently toxic to ethically administer to healthy volunteers, the initial human testing is often conducted in subjects. |
| |
● |
Phase 2. The biological product is evaluated in a limited patient population to identify possible adverse effects and safety risks, to preliminarily evaluate the efficacy of the product for specific targeted diseases and to determine dosage tolerance, optimal dosage and dosing schedule. |
| |
|
|
| |
● |
Phase 3. Clinical trials are undertaken to further evaluate dosage, clinical efficacy, potency, and safety in an expanded patient population at geographically dispersed clinical trial sites. These clinical trials are intended to establish the overall risk to benefit ratio of the product and provide an adequate basis for product labeling. |
Post-approval clinical trials,
sometimes referred to as Phase 4 clinical trials, may be conducted after initial marketing approval. These clinical trials are used to
gain additional experience from the treatment of patients in the intended therapeutic indication, particularly for long-term safety follow-up.
After the completion of clinical
trials of a biological product, FDA approval of a BLA must be obtained before commercial marketing of the biological product. The BLA
must include results of product development, laboratory and animal studies, human trials, information on the manufacture and composition
of the product, proposed labeling and other relevant information. The FDA may grant deferrals for submission of data, or full or partial
waivers. The testing and approval processes require substantial time and effort and there can be no assurance that the FDA will accept
the BLA for filing and, even if filed, that any approval will be granted on a timely basis, if at all. Before approving a BLA, the FDA
will inspect the facilities at which the product is manufactured. The FDA will not approve the product unless it determines that the manufacturing
processes and facilities are in compliance with cGMP requirements and adequate to assure consistent production of the product within required
specifications. Additionally, before approving a BLA, the FDA will typically inspect one or more clinical sites to assure that the clinical
trials were conducted in compliance with IND trial requirements and GCP requirements. To assure cGMP and GCP compliance, an applicant
must incur significant expenditure of time, money and effort in the areas of training, record keeping, production, and quality control.
Notwithstanding the submission
of relevant data and information, the FDA may ultimately decide that the BLA does not satisfy its regulatory criteria for approval and
deny approval. Data obtained from clinical trials are not always conclusive and the FDA may interpret data differently than we interpret
the same data. We cannot predict with any certainty if or when we might submit a BLA for regulatory approval for our product candidates
or whether any such BLA will be approved by the FDA. Human clinical trials are very expensive and difficult to design and implement, in
part because they are subject to rigorous regulatory requirements. For example, the FDA may not agree with our proposed endpoints for
any clinical trial we propose, which may delay the commencement of our clinical trials. The clinical trial process is also lengthy and
requires substantial time and effort.
In December 2015, the FDA
cleared our IND filing for Iomab-B and we have completed patient enrollment of a randomized, controlled, pivotal Phase 3 clinical trial
under such IND to study Iomab-B in patients 55 years of age or older with relapsed or refractory AML. The Phase 3 SIERRA trial met its
primary endpoint with high statistical significance with positive results for secondary endpoints and exploratory endpoints and it is
expected to form the basis for a BLA for Iomab-B for use in preparing and conditioning AML patients for a BMT. Additionally, there are
physician IND trials at the FHCRC that have been conducted or are currently ongoing at FHCRC with Iomab-B (for other target indications)
and the apamistamab antibody (formerly known as BC8) we licensed. We have other clinical trials ongoing and others that we have planned
but not-yet commenced, for our other drug candidate Actimab-A under our own sponsorship and investigator-initiated trials ongoing. Except
for Iomab-B (for patients with AML), we expect that the clinical trials we need to conduct to be in a position to submit BLAs for our
product candidates currently in-development will take, at least, several years to complete. Moreover, failure can occur at any stage of
the trials, and we could encounter problems that cause us to abandon or repeat clinical trials. Also, the results of early preclinical
and clinical testing may not be predictive of the results of subsequent clinical trials. A number of companies in the biopharmaceutical
industry have suffered significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding
promising results in earlier studies. And, preclinical and clinical data are often susceptible to multiple interpretations and analyses.
Many companies that have believed their product candidates performed satisfactorily in preclinical studies and clinical trials have, nonetheless,
failed to obtain marketing approval of their products. Success in preclinical testing and early clinical trials does not ensure that later
clinical trials, which involve many more subjects, and the results of later clinical trials may not replicate the results of prior clinical
trials and preclinical testing. Any failure or substantial delay in our product development plans may have a material adverse effect on
our business.
We may encounter substantial delays in our
clinical trials or may not be able to conduct our trials on the timelines we expect.
We cannot predict whether
we will encounter problems with any of our ongoing or planned clinical trials that will cause us or regulatory authorities to delay, suspend,
or discontinue clinical trials or to delay the analysis of data from ongoing clinical trials. Any of the following could delay or disrupt
the clinical development of our product candidates and potentially cause our product candidates to fail to receive regulatory approval:
| |
● |
conditions imposed on us by the FDA or comparable foreign authorities regarding the scope or design of our clinical trials; |
| |
|
|
| |
● |
delays in receiving, or the inability to obtain, required approvals from IRBs or other reviewing entities at clinical sites selected for participation in our clinical trials; |
| |
|
|
| |
● |
delays in enrolling patients into clinical trials; |
| |
|
|
| |
● |
a lower than anticipated retention rate of patients in clinical trials; |
| |
|
|
| |
● |
the need to repeat or discontinue clinical trials as a result of inconclusive or negative results or unforeseen complications in testing or because the results of later trials may not confirm positive results from earlier preclinical studies or clinical trials; |
| |
|
|
| |
● |
inadequate supply, delays in distribution, deficient quality of, or inability to purchase or manufacture drug product, comparator drugs or other materials necessary to conduct our clinical trials; |
| |
● |
unfavorable FDA or other foreign regulatory inspection and review of a clinical trial site or records of any clinical or preclinical investigation; |
| |
|
|
| |
● |
serious and unexpected drug-related side effects experienced by participants in our clinical trials, which may occur even if they were not observed in earlier trials or only observed in a limited number of participants; |
| |
|
|
| |
● |
a finding that the trial participants are being exposed to unacceptable health risks; |
| |
|
|
| |
● |
the placement by the FDA or a foreign regulatory authority of a clinical hold on a trial; or |
| |
|
|
| |
● |
delays in obtaining regulatory agency authorization for the conduct of our clinical trials. |
We may suspend, or the FDA
or other applicable regulatory authorities may require us to suspend, clinical trials of a product candidate at any time if we or they
believe the patients participating in such clinical trials, or in independent third-party clinical trials for drugs based on similar technologies,
are being exposed to unacceptable health risks including but not limited to unacceptable or suboptimal factors related to toxicity, clinical
efficacy, imbalances in safety and efficacy profiles or for other reasons.
Further, individuals involved
with our clinical trials may serve as consultants to us from time to time and receive stock options or cash compensation in connection
with such services. If these relationships and any related compensation to the clinical investigator carrying out the study result in
perceived or actual conflicts of interest, or the FDA concludes that the financial relationship may have affected interpretation of the
study, the integrity of the data generated at the applicable clinical trial site may be questioned and the utility of the clinical trial
itself may be jeopardized. The delay, suspension or discontinuation of any of our clinical trials, or a delay in the analysis of clinical
data for our product candidates, for any of the foregoing reasons, could adversely affect our efforts to obtain regulatory approval for
and to commercialize our product candidates, increase our operating expenses and have a material adverse effect on our financial results.
Clinical trials may also be
delayed or terminated as a result of ambiguous or negative interim results. In addition, a clinical trial may be suspended or terminated
by us, the FDA, the IRBs at the sites where the IRBs are overseeing a trial, or a data safety monitoring board, or DSMB (Data Safety Monitoring
Board)/DMC (Data Monitoring Committee), overseeing the clinical trial at issue, or other regulatory authorities due to a number of factors,
including:
| |
● |
failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols; |
| |
● |
inspection of the clinical trial operations or trial sites by the FDA or other regulatory authorities resulting in the imposition of a clinical hold; |
| |
● |
varying interpretation of data by the FDA or similar foreign regulatory authorities; |
| |
● |
failure to achieve primary or secondary endpoints or other failure to demonstrate efficacy; |
| |
● |
unforeseen safety issues; or |
| |
● |
lack of adequate funding to continue the clinical trial. |
Modifications to our product candidates
may require federal approvals.
The BLA application is the
vehicle through which the company may formally propose that the FDA approve a new pharmaceutical for sale and marketing in the United
States. Once a particular product candidate receives FDA approval, expanded uses or uses in new indications of our products may require
additional human clinical trials and new regulatory approvals, including additional IND and BLA submissions and premarket approvals before
we can begin clinical development, and/or prior to marketing and sales. If the FDA requires new approvals for a particular use or indication,
we may be required to conduct additional clinical studies, which would require additional expenditures and harm our operating results.
If the products are already being used for these new indications, we may also be subject to significant enforcement actions.
Conducting clinical trials
and obtaining approvals is a time-consuming process, and delays in obtaining required future approvals could adversely affect our ability
to introduce new or enhanced products in a timely manner, which in turn would have an adverse effect on our business prospects, financial
condition and results of operation.
Clinical trials necessary to support approval
of our product candidates are time-consuming and expensive.
Initiating and completing
clinical trials necessary to support FDA approval of a BLA for Iomab-B, Actimab-A, and other product candidates, is a time-consuming and
expensive process, and the outcome is inherently uncertain. Moreover, the results of early clinical trials are not necessarily predictive
of future results, and any product candidate we advance into clinical trials may not have favorable results in later clinical trials.
We worked with the FDA to develop the SIERRA clinical trial to test the safety and efficacy of Iomab-B in patients with relapsed or refractory
AML who are age 55 and above prior to a BMT. This trial is designed to support a BLA filing for marketing approval by the FDA. In addition
to clinical data, a BLA filing encompasses preclinical, CMC, labeling and other information. Even if the clinical data from the SIERRA
trial is positive, there can be no assurances that the BLA filing we produce will meet all of the FDA’s requirements or that they
will not request additional information or studies, which may delay the FDA’s review or we may not be able to produce. We have also
worked with the FDA to develop a regulatory pathway for lintuzumab-Ac-225 in patients with high-risk MDS that consists of a dose-confirming
Phase 1 trial that can be followed by a randomized, controlled pivotal trial that could support a BLA filing. To date, we have not initiated
this clinical trial and we may never elect or be able to do so. There can be no assurance that the data generated during the trial, or
any trial, will meet our chosen safety and effectiveness endpoints or otherwise produce results that will eventually support the filing
or approval of a BLA. Even if the data from this trial are favorable, the data may not be predictive of the results of any future clinical
trials.
Preliminary, Interim, and “top-line”
data from our clinical trials that we announce or publish from time to time may change as more patient data become available and are subject
to audit and verification procedures that could result in material changes in the final data.
From time to time, we
may publicly disclose preliminary, interim, and top-line data from our clinical trials, which is based on a preliminary analysis of then-available
data, and the results and related findings and conclusions are subject to change as more patient data become available or following a
more comprehensive review of the data related to the particular study or trial. For example, in February 2023 we announced that Iomab-B
met the primary endpoint of dCR in the SIERRA trial with statistical significance (p<0.0001) producing a durable Complete Response
rate of 22% compared to a 0% durable Complete Response rate in the control arm. We may also make assumptions, estimations, calculations
and conclusions as part of our analyses of data, and we may not have received or had the opportunity to fully and carefully evaluate all
data. Our clinical trials may be open label studies and certain of our clinical development and or operations staff may review interim
or preliminary safety or efficacy data during routine data collection, cleaning and analysis from time to time. Interim or preliminary
results that we report may differ from future results of the same studies, or different conclusions or considerations may qualify such
results once additional data have been received and fully evaluated. Preliminary, interim or top-line data also remain subject to audit
and verification procedures that may result in the final data being materially different from the top-line, interim or preliminary data
we previously published. As a result, top-line, interim and preliminary data should be viewed with caution until the final data are available.
From time to time, we may
also disclose interim data from our preclinical studies and clinical trials. Interim data from clinical trials that we may complete are
subject to the risk that one or more of the clinical outcomes may materially change as patient enrollment continues and more patient data
become available. Adverse differences between interim data and final data could significantly harm our business prospects. Further, disclosure
of interim data by us or by our competitors could result in volatility in the price of our common stock.
Further, others, including
regulatory agencies, may not accept or agree with our assumptions, estimates, calculations, conclusions or analyses or may interpret or
weigh the importance of data differently, which could impact the value of the particular program, the approvability or commercialization
of the particular product candidate or product and our company in general. In addition, the information we choose to publicly disclose
regarding a particular study or clinical trial is based on what is typically extensive information, and you or others may not agree with
what we determine is material or otherwise appropriate information to include in our disclosure.
If the interim, top-line or
preliminary data that we report differ from final results, or if others, including regulatory authorities, disagree with the conclusions
reached, our ability to obtain approval for, and commercialize, our product candidates may be harmed, which could harm our business, operating
results, prospects or financial condition.
Our clinical trials may fail to demonstrate
adequately the efficacy and safety of our product candidates, which would prevent or delay regulatory approval and commercialization.
Even if our clinical trials
are completed as planned, we cannot be certain that their results will support our product candidate claims or that the FDA or foreign
authorities will agree with our conclusions regarding them. Success in pre-clinical studies and early clinical trials does not ensure
that later clinical trials will be successful, and we cannot be sure that the later trials will replicate the results of prior trials
and pre-clinical studies. The clinical trial process may fail to demonstrate that our product candidates are safe and effective for the
proposed indicated uses. If FDA concludes that the clinical trials for Iomab-B, Actimab-A, or any other product candidate for which we
might seek approval, have failed to demonstrate safety and effectiveness, we would not receive FDA approval to market that product candidate
in the United States for the indications sought. In addition, such an outcome could cause us to abandon the product candidate and might
delay development of others. Any delay or termination of our clinical trials will delay or preclude the filing of any submissions with
the FDA and, ultimately, our ability to commercialize our product candidates and generate revenues. It is also possible that patients
enrolled in clinical trials will experience adverse side effects that are not currently part of a product candidate’s profile.
The intellectual property related to antibodies
we have licensed has expired or likely expired.
The key patents related to
the humanized antibody, lintuzumab, which we use in our Actimab-A product candidate have expired. It is generally possible that others
may be eventually able to use an antibody with the same sequence, and we will then need to rely on additional patent protection covering
alpha particle drug products comprising Ac-225. Our final drug construct, Actimab A, consists of the lintuzumab antibody labeled with
the isotope Ac-225. We currently own issued and pending patents relating to methods of manufacturing Actimab-A, methods of treatment using
Actimab-A and production of the Ac-225 isotope. In addition, we possess trade secrets and know how related to the manufacturing and use
of isotopes. Any competing product based on the lintuzumab antibody is likely to require several years of development before achieving
our product candidate’s current status and may be subject to significant regulatory hurdles but such development by others is nevertheless
a possibility that could negatively impact our business in the future. We own 4 issued U.S. patents, 1 issued Canadian patent, 1 issued
European patent (validated as a national patent in several countries) and 1 issued Japanese patent that relate to the composition of our
Iomab-B product candidate. Patent applications relating to Iomab-B are also pending in the U.S. and internationally. We have and may continue
to file patents related to Iomab-B that can provide barriers to entry but there is no certainty that these patents will be granted or
such granting thereof will adequately prevent others from seeking to replicate and use the apamistamab antibody or the construct. Our
patent portfolio includes pending applications related to radioimmunoconjugate composition, formulation administration, and methods of
use in treating solid or liquid cancers. This subject matter includes composition, administration, and methods of treatment for our product
candidates Actimab-A and Iomab-B. Any competing product based on the antibody used in Iomab-B is likely to require several years of development
before achieving our product candidate’s current status and may be subject to significant regulatory hurdles but such development
by others is nevertheless a possibility that could negatively impact our business in the future.
Our CD33 program clinical trials are testing
the same drug construct.
Our CD33 program is comprised
of several ongoing and planned clinical trials including investigator-initiated trials in AML studying the same drug construct consisting
of lintuzumab-Ac-225. Negative results from any of these trials could negatively impact our ability to enroll or complete our other trials
studying lintzumab-Ac-225 including future studies conducted under our CRADA with the NCI. Additionally, negative outcomes including safety
concerns, may result in the FDA discontinuing other trials utilizing lintuzumab-Ac-225.
We may be unable to obtain a sufficient
supply of isotopes to support clinical development or at commercial scale.
Iodine-131 is a key component
of our Iomab-B drug candidate. We currently source medical grade I-131 from three suppliers including two leading global manufacturers.
Currently, there is sufficient supply of I-131 to support additional trials we may undertake utilizing I-131 and for commercialization
of Iomab-B. We continually evaluate I-131 manufacturers and suppliers and intend to have multiple qualified suppliers prior to the commercial
launch of Iomab-B. While we consider I-131 to be commoditized and obtainable through several suppliers, there can be no guarantee that
we will be able to secure I-131 or obtain I-131 on terms that are acceptable to us.
Actinium-225 is a key component
of our Actimab-A product candidate, technology platform, preclinical R&D programs and other drug candidates that we might consider
for development with the Ac-225 payload. There are adequate quantities of Ac-225 available today to meet our current needs via our present
supplier, the Department of Energy (“DOE”). The Ac-225 currently supplied to Actinium’s clinical trials from the DOE
is derived from the natural decay of thorium-229 from so-called ‘thorium-cows’ and is able to produce sufficient quantities
that are several multiples of the amount of Ac-225 we require to supply our clinical programs through to early commercialization phase.
The DOE is also producing Ac-225 from a recently developed alternative route for Ac-225 production via a linear accelerator that is currently
being evaluated by Actinium. Initial preclinical and modelling results have indicated that the linear accelerator sourced Ac-225 does
not impact labelling efficiency and expected distribution. In accordance with representations made by the DOE, the capacity of Ac-225
from this route is expected to be sufficient to supply all of Actinium’s pipeline and commercial Ac-225 needs and support new program
expansion by not just Actinium but also other companies that are developing Ac-225 based products. Additional routes of Ac-225 production
are being pursued by the DOE including the generation of new thorium cows and production via a cyclotron. The cyclotron production method
for Ac-225 production leverages Actinium’s proprietary technology and know-how and presents an additional path towards production
of high-quality Ac-225 at a scale that would be able to satisfy commercial needs. In addition, we are aware of at least ten other government
and non-government entities globally including the U.S., Canada, Russia, Belgium, France and Japan that have, or expect to have ability
to supply Ac-225 or equipment for its production within the timeframes relevant to the potential first commercial approval of our Ac-225-based
drug candidate.
Our contract for supply of
this isotope from the DOE must be renewed yearly, and we renewed our contract to extend through the end of 2023. While we expect this
contract will continue to be renewed at the end of its term as it has since 2009, there can be no assurance that the DOE will renew the
contract or that change its policies that allow for the sale of isotope to us. Failure to acquire sufficient quantities of medical grade
Ac-225 would make it impossible to effectively complete clinical trials and to commercialize any Ac-225 based drug candidates that we
may develop and would materially harm our business.
Our ability to conduct clinical
trials to advance our drug candidates is dependent on our ability to obtain the radioisotopes I-131, Ac-225 and other isotopes we may
choose to utilize in the future. Currently, we are dependent on third party manufacturers and suppliers for our isotopes. These suppliers
may not perform their contracted services or may breach or terminate their agreements with us. Our suppliers are subject to regulations
and standards that are overseen by regulatory and government agencies and we have no control over our suppliers’ compliance to these
standards. Failure to comply with regulations and standards may result in their inability to supply isotopes and could result in delays
in our clinical trials, which could have a negative impact on our business. We have developed intellectual property, know-how and trade
secrets related to the manufacturing process of Ac-225. While we have manufactured medical grade Ac-225 of a purity compared to the cyclotron
sourced material in the past, this activity was terminated due to operating cost reasons and we currently do not have experience in manufacturing
medical grade Ac-225 and may not obtain the resources necessary to establish our own manufacturing capabilities in future. Our inability
to build out and establish our own manufacturing facilities would require us to continue to rely on third party suppliers as we currently
do. However, based on our current third-party suppliers and potential future suppliers of Ac-225 we expect to have adequate isotope supply
to support our current ongoing clinical trials, current and planned preclinical R&D activities and commercialization should our drug
candidates receive regulatory approval.
If we encounter difficulties enrolling patients
in our clinical trials, our clinical development activities could be delayed or otherwise adversely affected.
The timely completion of clinical
trials in accordance with their protocols depends on our ability to enroll a sufficient number of patients who remain in the trial until
its conclusion. We may experience difficulties in patient enrollment in our clinical trials for a variety of reasons, including:
| |
● |
the size and nature of the patient population; |
| |
● |
the patient eligibility criteria defined in the protocol; |
| |
● |
the size of the study population required for analysis of the trial’s primary endpoints; |
| |
● |
the proximity of patients to trial sites; |
| |
● |
the design of the trial; |
| |
● |
our ability to recruit clinical trial investigators with the appropriate competencies and expertise; |
| |
● |
competing clinical trials for similar or alternate therapeutic treatments; |
| |
● |
clinician’s and patients’ perceptions as to the potential advantages and side effects of the product candidate being studied in relation to other available therapies; |
| |
● |
our ability to obtain and maintain patient consents; and |
| |
● |
the risk that patients enrolled in clinical trials will not complete a clinical trial. |
In addition, refractory patients,
which several of our trials are enrolling, participating in clinical trials are seriously and often terminally ill and therefore may not
complete the clinical trial due to reasons including comorbid conditions or occurrence of adverse medical events related or unrelated
to the investigational products, or death. Even if we are able to enroll a sufficient number of patients in our clinical trials, delays
in patient enrollment will result in increased costs or affect the timing of our planned trials, which could adversely affect our ability
to advance the development of our product candidates.
FDA may take actions that would prolong,
delay, suspend, or terminate clinical trials of our product candidates, which may delay or prevent us from commercializing our product
candidates on a timely basis.
There can be no assurance
that the data generated in our clinical trials will be acceptable to FDA or that if future modifications during the trial are necessary,
that any such modifications will be acceptable to FDA. Certain modifications to a clinical trial protocol made during the course of the
clinical trial have to be submitted to the FDA. This could result in the delay or halt of a clinical trial while the modification is evaluated.
In addition, depending on the quantity and nature of the changes made, FDA could take the position that some or all of the data generated
by the clinical trial is not usable because the same protocol was not used throughout the trial. This might require the enrollment of
additional subjects, which could result in the extension of the clinical trial and the FDA delaying approval of a product candidate. If
the FDA believes that its prior approval is required for a particular modification, it can delay or halt a clinical trial while it evaluates
additional information regarding the change.
Any delay or termination of
our current or future clinical trials as a result of the risks summarized above, including delays in obtaining or maintaining required
approvals from IRBs, delays in patient enrollment, the failure of patients to continue to participate in a clinical trial, and delays
or termination of clinical trials as a result of protocol modifications or adverse events during the trials, may cause an increase in
costs and delays in the filing of any submissions with the FDA, delay the approval and commercialization of our product candidates or
result in the failure of the clinical trial, which could adversely affect our business, operating results and prospects. Lengthy delays
in the completion of our Iomab-B clinical trials would adversely affect our business and prospects and could cause us to cease operations.
We have obtained orphan drug designation
from FDA for two of our current product candidates and intend to pursue such designation for other candidates and indications in the future,
but we may be unable to obtain such designations or to maintain the benefits associated with any orphan drug designations we have received
or may receive in the future.
We have received orphan drug
designation for Iomab-B and Actimab-A for treatment of AML in both the United States and the EU. Under the Orphan Drug Act, the FDA may
grant orphan designation to a drug or biologic intended to treat a rare disease or condition, which is a disease or condition that affects
fewer than 200,000 individuals in the United States, or if it affects more than 200,000 individuals in the United States, there is no
reasonable expectation that the cost of developing and making available a drug or biologic for this type of disease or condition will
be recovered from sales in the United States for that drug or biologic. Similarly, the EMA grants orphan drug designation to promote the
development of products that are intended for the diagnosis, prevention, or treatment of a life-threatening or chronically debilitating
condition affecting not more than five in 10,000 persons in the EU.
Orphan drug designation neither
shortens the development time or regulatory review time of a drug or biologic nor gives the drug or biologic any advantage in the regulatory
review or approval process. In the United States, orphan drug designation entitles a party to financial incentives, such as opportunities
for grant funding towards clinical trial costs, tax advantages, and application fee waivers. In addition, if a product candidate receives
the first FDA approval for the indication for which it has orphan designation, such product is entitled, upon approval, to seven years
of orphan-drug exclusivity, during which the FDA may not approve any other application to market the same drug for the same indication,
unless a subsequently approved product is clinically superior to orphan drug or where the manufacturer is unable to assure sufficient
product quantity in the applicable patient population. In the EU, orphan drug designation entitles a party to financial incentives such
as reduction of fees or fee waivers and ten years of market exclusivity following drug or biological product approval. This period may
be reduced to six years if the orphan drug designation criteria are no longer met, including where it is shown that the product is sufficiently
profitable not to justify maintenance of market exclusivity.
Even if we obtain (or have
obtained) orphan drug designation for certain product candidates, we may not be the first to obtain marketing approval for such candidates
for the applicable indications due to the uncertainties inherent in the development of novel biologic products. And, an orphan drug candidate
may not receive orphan-drug exclusivity upon approval if such candidate is approved for a use that is broader than the indication for
which it received orphan designation. In addition, exclusive marketing rights in the United States may be lost if the FDA later determines
that the request for designation was materially defective or if the manufacturer is unable to assure sufficient quantities of the product
to meet the needs of patients with the rare disease or condition.
Finally, even if we successfully
obtain orphan-drug exclusivity for an orphan drug candidate upon approval, such exclusivity may not effectively protect the product from
competition because (i) different drugs with different active moieties can be approved for the same condition; and (ii) the FDA or EMA
can also subsequently approve a subsequent product with the same active moiety and for the same indication as the orphan drug if the later-approved
drug if deemed clinically superior to the orphan drug.
Even if we receive regulatory approval of
our product candidates, we will be subject to ongoing regulatory obligations and continued regulatory review.
Any regulatory approvals that
we receive for our product candidates will require surveillance to monitor the safety and efficacy of the product candidate. The FDA may
also require a REMS in order to approve our product candidates, which could entail requirements for a medication guide, physician communication
plans or additional elements to ensure safe use, such as restricted distribution methods, patient registries and other risk minimization
tools. In addition, if the FDA or a comparable foreign regulatory authority approves our product candidates, the manufacturing processes,
labeling, packaging, distribution, adverse event reporting, storage, advertising, promotion, import, export and recordkeeping for our
product candidates will be subject to extensive and ongoing regulatory requirements. These requirements include submissions of safety
and other post-marketing information and reports, registration, as well as continued compliance with cGMPs and GCPs for any clinical trials
that we conduct post-approval. In addition, the FDA could require us to conduct another study to obtain additional safety or biomarker
information. Later discovery of previously unknown problems with our product candidates, including adverse events of unanticipated severity
or frequency, or with our third-party suppliers or manufacturing processes, or failure to comply with regulatory requirements, may result
in, among other things:
| |
● |
restrictions on the marketing or manufacturing of our product candidates, withdrawal of the product from the market, or voluntary or mandatory product recalls; |
| |
● |
fines, warning letters or holds on clinical trials; |
| |
● |
refusal by the FDA to approve pending applications or supplements to approved applications filed by us or suspension or revocation of license approvals; |
| |
● |
product seizure or detention, or refusal to permit the import or export of our product candidates; and |
| |
● |
injunctions or the imposition of civil or criminal penalties. |
The FDA’s and other
regulatory authorities’ policies may change, and additional government regulations may be enacted that could prevent, limit or delay
regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of government regulation that may arise
from future legislation or administrative action, either in the United States or abroad. If we are slow or unable to adapt to changes
in existing requirements or the adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we
may lose any marketing approval that we may have obtained, and we may not achieve or sustain profitability.
Coverage and reimbursement may be limited
or unavailable in certain market segments for our product candidates which could limit our sales of our product candidates, if approved.
The commercial success of
our product candidates in both domestic and international markets will be substantially dependent on whether third-party coverage and
reimbursement is available for patients that use our products. However, the availability of insurance coverage and reimbursement for newly
approved cancer therapies is uncertain, and therefore, third-party coverage may be particularly difficult to obtain even if our products
are approved by the FDA as safe and efficacious. Patients using existing approved therapies are generally reimbursed all or part of the
product cost by Medicare or other third-party payors. Medicare, Medicaid, health maintenance organizations and other third-party payors
are increasingly attempting to contain healthcare costs by limiting both coverage and the level of reimbursement of new drugs, and, as
a result, they may not cover or provide adequate payment for these products. Submission of applications for reimbursement approval generally
does not occur prior to the filing of a BLA for that product and may not be granted until many months after BLA approval. In order to
obtain coverage and reimbursement for these products, we or our commercialization partners may have to agree to a net sales price lower
than the net sales price we might charge in other sales channels. The continuing efforts of government and third-party payors to contain
or reduce the costs of healthcare may limit our revenue. Initial dependence on the commercial success of our products may make our revenues
particularly susceptible to any cost containment or reduction efforts.
Healthcare legislative reform measures intended
to increase pressure to reduce prices of pharmaceutical products paid for by Medicare or, otherwise, affect the federal regulation of
the U.S. healthcare system could have a material adverse effect our business, future revenue, if any, and results of operations.
In the United States, there
have been a number of legislative and regulatory initiatives focused on containing the cost of healthcare. The Affordable Care Act, for
example, substantially changed the way healthcare is financed by both governmental and private insurers. The Affordable Care Act contains
a number of provisions that could impact our business and operations, primarily, once we obtain FDA approval to commercialize one of our
product candidates in the United States, if ever, and may also affect our operations in ways we cannot currently predict. Affordable Care
Act provisions that may affect our business include, among others, those governing enrollment in federal healthcare programs, reimbursement
changes, rules regarding prescription drug benefits under health insurance exchanges, expansion of the 340B program, expansion of state
Medicaid programs, fees and increased discount and rebate obligations, transparency and reporting requirements, and fraud and abuse enforcement.
Such changes may impact existing government healthcare programs, industry competition, formulary composition, and may result in the development
of new programs, including Medicare payment for performance initiatives, health technology assessments, and improvements to the physician
quality reporting system and feedback program.
There have been significant
judicial, administrative, executive, and legislative initiatives to modify, limit, replace, or repeal the Affordable Care Act since its
enactment. For example, former President Trump issued several Executive Orders and other directives designed to delay the implementation
of certain provisions of the Affordable Care Act or otherwise circumvent some of the requirements for health insurance mandated by the
Affordable Care Act. Concurrently, Congress considered legislation that would repeal or replace all or part of the Affordable Care Act.
While Congress has not passed comprehensive repeal legislation, several bills affecting the implementation the Affordable Care Act have
been passed. For example, the Tax Cuts and Jobs Act of 2017 eliminated the Affordable Care Act provision requiring individuals to purchase
and maintain health coverage, or the “individual mandate,” by reducing the associated penalty to zero, beginning in 2019.
In December 2018, a district court in Texas held that the individual mandate is unconstitutional and that the rest of the Affordable Care
Act is, therefore, invalid. On appeal, the Fifth Circuit Court of Appeals affirmed the holding on the individual mandate but remanded
the case back to the lower court to reassess whether and how such holding affects the validity of the rest of the Affordable Care Act.
The Fifth Circuit’s decision on the individual mandate was appealed to the U.S. Supreme Court. On June 17, 2021, the Supreme Court
held that the plaintiffs (comprised of the state of Texas, as well as numerous other states and certain individuals) did not have standing
to challenge the constitutionality of the Affordable Care Act’s individual mandate and, accordingly, vacated the Fifth Circuit’s
decision and instructed the district court to dismiss the case. As a result, the Affordable Care Act will remain in-effect in its current
form for the foreseeable future; however, we cannot predict what additional challenges may arise in the future, the outcome thereof, or
the impact any such actions may have on our business.
In addition to the Affordable
Care Act, there have been numerous other Congressional initiatives and proposed and enacted federal and state legislation designed to,
among other things, bring more transparency to drug pricing, review the relationship between pricing and manufacturer patient programs,
and reform government program reimbursement methodologies for drug products. Pharmaceutical product prices have been the focus of increased
scrutiny by the government, including certain state attorneys general, members of Congress and the United States Department of Justice.
State or federal healthcare reform measures or other social or political pressure to lower the cost of pharmaceutical products could have
a material adverse impact on our business, results of operations and financial condition.
The Biden administration also
introduced various measures in 2021 focusing on healthcare and drug pricing, in particular. For example, on January 28, 2021, President
Biden issued an executive order that initiated a special enrollment period for purposes of obtaining health insurance coverage through
the Affordable Care Act marketplace, which began on February 15, 2021, and remained open through August 15, 2021. The executive order
also instructed certain governmental agencies to review and reconsider their existing policies and rules that limit access to healthcare,
including among others, reexamining Medicaid demonstration projects and waiver programs that include work requirements and policies that
create unnecessary barriers to obtaining access to health insurance coverage through Medicaid or the Affordable Care Act. On the legislative
front, the American Rescue Plan Act of 2021 was signed into law on March 11, 2021, which, in relevant part, eliminates the statutory Medicaid
drug rebate cap, currently set at 100% of a drug’s average manufacturer price, for single source drugs and innovator multiple source
drugs, beginning January 1, 2024. And, in July 2021, the Biden administration released an executive order entitled, “Promoting Competition
in the American Economy,” with multiple provisions aimed at prescription drugs. In response, on September 9, 2021, HHS released
a “Comprehensive Plan for Addressing High Drug Prices” that outlines principles for drug pricing reform and sets out a variety
of potential legislative policies that Congress could pursue as well as potential administrative actions HHS can take to advance these
principles.
Most recently, on August 16,
2022, President Biden signed into law the Inflation Reduction Act of 2022 (the “IRA”), which, among other
provisions, included several measures intended to lower the cost of prescription drugs and related healthcare reforms. Specifically, the
IRA authorizes and directs the Department of Health and Human Services (the “DHHS”) to set drug price caps for certain high-cost
Medicare Part B and Part D qualified drugs, with the initial list of drugs to be selected by September 1, 2023, and the first year of
maximum price applicability to begin in 2026. The IRA further authorizes the DHHS to penalize pharmaceutical manufacturers that increase
the price of certain Medicare Part B and Part D drugs faster than the rate of inflation. Finally, the IRA creates significant changes
to the Medicare Part D benefit design by capping Part D beneficiaries’ annual out-of-pocket spending at $2,000 beginning in 2025.
We cannot be sure whether additional or related legislation or rulemaking will be issued or enacted, or what impact, if any, such changes
will have on the profitability of any of our drug candidates, if approved for commercial use, in the future.
Our relationships with customers, health
care professionals and third-party payors may be subject to applicable healthcare laws, which could expose us to penalties, including
administrative, civil or criminal penalties, damages, fines, imprisonment, exclusion from participation in federal healthcare programs
such as Medicare and Medicaid, reputational harm, the curtailment or restructuring of our operations and diminished future profits and
earnings.
Healthcare professionals and
third-party payors will play a primary role in the recommendation and prescription of any product candidates for which we obtain marketing
approval. Our current and future arrangements with customers, healthcare professionals and third-party payors may expose us to broadly
applicable fraud and abuse and other healthcare laws and regulations that may constrain the business or financial arrangements and relationships
through which we conduct research, market, sell and distribute any products for which we obtain marketing approval. Federal and state
healthcare laws and regulations that may affect our operations, directly or indirectly, include the following, among others:
| |
● |
the federal Anti-Kickback Statute, which prohibits persons and entities from, among other things, knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in cash or in kind, to induce or reward either the referral of an individual for, or the purchase, lease, order or recommendation of, any good, facility, item or service, for which payment may be made under federal and state healthcare programs such as Medicare and Medicaid; |
| |
● |
the federal false claims laws, including civil whistleblower or qui tam actions under the federal False Claims Act, which impose criminal and civil penalties against individuals or entities for, among other things, knowingly presenting, or causing to be presented, to the federal government, claims for payment that are false or fraudulent or making a false statement to avoid, decrease or conceal an obligation to pay money to the federal government; |
| |
● |
the federal Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH, which imposes criminal and civil liability for, among other things, executing a scheme to defraud any healthcare benefit program or making false statements relating to healthcare matters and also imposes obligations, including mandatory contractual terms, on covered entities, including certain healthcare providers, health plans, and healthcare clearinghouses, and their respective business associates that create, receive, maintain or transmit individually identifiable health information for or on behalf of the covered entity as well as their covered subcontractors, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
| |
● |
the federal Civil Monetary Penalties Law, which prohibits, among other things, the offering or transfer of remuneration to a Medicare or state healthcare program beneficiary if the person knows or should know it is likely to influence the beneficiary’s selection of a particular provider, practitioner, or supplier of services reimbursable by Medicare or a state healthcare program, unless an exception applies; |
| |
● |
the federal Physician Payments Sunshine Act, created under the Affordable Care Act, and its implementing regulations, which requires certain manufacturers of drugs, devices, biologicals and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to report annually information related to certain payments or other transfers of value provided to physicians and any ownership and investment interests held by physicians or their immediate family members. Beginning in 2022, applicable manufacturers also will be required to report such information regarding payments and other transfers of value to physician assistants, nurse practitioners, clinical nurse specialists, anesthesiologist assistants, certified registered nurse anesthetists and certified nurse midwives during the previous year; and |
| |
● |
analogous state laws and regulations, including (among others) state anti-kickback and false claims laws, which may apply to our business practices, including, but not limited to, research, distribution, sales and marketing arrangements and claims involving healthcare items or services reimbursed by any third-party payor, including private insurers; state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the United States federal government, or otherwise restrict payments that may be made to healthcare providers and other potential referral sources; state laws and regulations that require drug manufacturers to file reports relating to pricing and marketing information and that require tracking gifts and other remuneration and items of value provided to healthcare professionals and entities; state and local laws that require the registration of pharmaceutical sales representatives; and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and often are not preempted by federal law, thus complicating compliance efforts. |
Efforts to comply with applicable
healthcare laws and regulations will involve substantial costs. Interpretations of standards of compliance under these laws and regulations
are rapidly changing and subject to varying interpretations and it is possible that governmental authorities will conclude that our business
practices may not comply with current or future statutes, regulations or case law involving applicable fraud and abuse or other healthcare
laws and regulations. If our operations are found to be in violation of any of these laws or any other laws that may apply to us, we may
be subject to significant civil, criminal and administrative penalties, damages, fines, exclusion from government funded healthcare programs,
such as Medicare and Medicaid, reputational harm, imprisonment, additional reporting obligations and oversight (if we become subject to
a corporate integrity agreement or other agreement to resolve allegations of non-compliance with these laws), and the curtailment or restructuring
of our operations, any of which could diminish our future profits or earnings. If any of the physicians or other providers or entities
with whom we expect to do business are found to be not in compliance with applicable laws, they may be subject to criminal, civil or administrative
sanctions, including exclusions from government funded healthcare programs.
Third-party payors may not adequately reimburse
customers for any product candidates that we may commercialize or promote, and may impose coverage restrictions or limitations such as
prior authorizations and step edits that affect their use.
Our ability to commercialize
any product candidates successfully also will depend in part on the extent to which coverage and adequate reimbursement for these products
and related treatments will be available from government health programs, private health insurers, integrated delivery networks and other
third-party payors. Third-party payors decide which medications they will pay for and establish reimbursement levels. A significant trend
in the United States healthcare industry and elsewhere is cost containment. Government authorities and third-party payors have attempted
to control costs by limiting coverage and the amount of payment for particular medications. Increasingly, third-party payors are requiring
that drug companies provide predetermined discounts from list prices and are challenging the prices charged for medical products. Coverage
and reimbursement may not be available for any product that we commercialize and, if reimbursement is available, the level of reimbursement
may not be sufficient for commercial success. Coverage and reimbursement may impact the demand for, or the price of, any product candidate
for which we obtain marketing approval. If coverage and reimbursement is not available or is available only to limited levels, we may
not be able to successfully commercialize any product candidate for which we obtain marketing approval.
Obtaining reimbursement approval
for any product candidate for which we obtain marketing approval from any government or other third-party payor is a time-consuming and
costly process. There may be significant delays in obtaining coverage and adequate reimbursement for newly approved products. Moreover,
eligibility for coverage and reimbursement does not imply that any product will be paid for in all cases or at a rate that covers our
costs, including research, development, manufacture, sale and distribution. Even when a payor determines that a product that we may commercialize
or promote is eligible for reimbursement under its criteria, the payor may impose coverage limitations that preclude payment for some
uses that are approved by the FDA, or may impose restrictions, such as prior authorization requirements, or may simply deny coverage altogether.
Interim reimbursement levels for new drugs, if applicable, may also not be sufficient to cover our costs and may not be made permanent.
Coverage and reimbursement rates may vary according to the use of the drug and the medical circumstances under which it is used may be
based on reimbursement levels already set for lower cost products or procedures or may be incorporated into existing payments for other
services. Net prices for drugs may be reduced by mandatory discounts or rebates required by government healthcare programs or private
payors and by any future relaxation of laws that presently restrict imports of drugs from countries where they may be sold at lower prices
than in the United States. Furthermore, the Centers for Medicare and Medicaid Services frequently change product descriptors, coverage
policies, product and service codes, payment methodologies and reimbursement values. Commercial third-party payors often rely upon Medicare
coverage policies and payment limitations in setting their own reimbursement policies. Our inability to promptly obtain and maintain coverage
and profitable payment rates from both government-funded programs and private payors for any approved products that we develop could have
a material adverse effect on our operating results, our ability to raise capital needed to commercialize our approved products and our
overall financial condition.
Risks Related to Third Parties
We rely on third parties to conduct our
clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines or comply with
regulatory requirements, we may not be able to obtain regulatory approval for or commercialize our product candidates.
We do not have the ability
to independently conduct our clinical trials for our product candidates and we must rely on third parties, such as contract research organizations,
medical institutions, clinical investigators and contract laboratories to conduct such trials. Our reliance on these third parties for
clinical development activities results in reduced control over these activities. Moreover, the FDA requires us to comply with regulations
and standards, commonly referred to as GCPs (good clinical practices), for conducting, recording and reporting the results of clinical
trials to assure that data and reported results are credible and accurate and that the trial participants are adequately protected. Our
reliance on third parties does not relieve us of these responsibilities and requirements. If we or any of our third-party contractors
fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA or comparable
foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot
assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials
complies with GCP regulations. In addition, our clinical trials must be conducted with product produced under current good manufacturing
practice, or cGMP, regulations. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay
the regulatory approval process.
If our consultants, contract
research organizations and other similar entities with which we are working do not successfully carry out their contractual duties, meet
expected deadlines, or comply with applicable regulations, we may be required to replace them. Although we believe that there are a number
of other third-party contractors we could engage to continue these activities, we may not be able to enter into arrangements with alternative
third-party contractors or to do so on commercially reasonable terms, which may result in a delay of our planned clinical trials and delayed
development of our product candidates.
In addition, our third-party
contractors are not our employees, and except for remedies available to us under our agreements with such third-party contractors, we
cannot control whether or not they devote sufficient time and resources to our programs. If these third parties do not successfully carry
out their contractual duties or regulatory obligations or meet expected deadlines, or if the quality or accuracy of the data they obtain
is compromised due to the failure to adhere to our clinical protocols or regulatory requirements or for other reasons, our pre-clinical
development activities or clinical trials may be extended, delayed, suspended or terminated, and we may not be able to obtain regulatory
approval for, or successfully commercialize, our product candidates on a timely basis, if at all, and our business, operating results
and prospects would be adversely affected.
The antibodies we use in our targeted radiotherapy
product candidates may be subject to generic competition.
We are not aware of any existing
or pending regulations or legislation that pertains to generic radiopharmaceutical products such as our targeted radiotherapy product
candidates. Our product candidates are regulated by the FDA as biologic products and we intend to seek approval for these products pursuant
to the BLA pathway. The Biologics Price Competition and Innovation Act of 2009, or BPCIA, created an abbreviated pathway for the approval
of biosimilar and interchangeable biologic products. The abbreviated regulatory pathway establishes legal authority for the FDA to review
and approve biosimilar biologics, including the possible designation of a biosimilar as “interchangeable” based on its similarity
to an existing brand product. Under the BPCIA, an application for a biosimilar product cannot be approved by the FDA until 12 years after
the original branded product was approved under a BLA. The law is complex and is still being interpreted and implemented by the FDA. As
a result, its ultimate impact, implementation, and meaning are subject to uncertainty. Even if a biosimilar gets approved for one of the
antibodies that we use, the final constructs of our drug candidates consist of an antibody, radioisotope and in some cases a linker. Therefore,
we do not believe that the final drug product of our candidates can be subject to competition from a biosimilar as outlined in BPCIA.
Our product candidates may never achieve
market acceptance.
Iomab-B, Actimab-A and future
product candidates that we may develop may never gain market acceptance among physicians, patients and the medical community. The degree
of market acceptance of any of our products will depend on a number of factors, including the actual and perceived effectiveness and reliability
of the product; the results of any long-term clinical trials relating to use of the product; the availability, relative cost and perceived
advantages and disadvantages of alternative technologies; the degree to which treatments using the product are approved for reimbursement
by public and private insurers; the strength of our marketing and distribution infrastructure; and the level of education and awareness
among physicians and hospitals concerning the product.
We believe that oncologists
and other physicians will not widely adopt a product candidate unless they determine, based on experience, clinical data, and published
peer-reviewed journal articles, that the use of that product candidate provides an effective alternative to other means of treating specific
cancers. Patient studies or clinical experience may indicate that treatment with our product candidates does not provide patients with
sufficient benefits in extension of life or quality of life. We believe that recommendations and support for the use of each product candidate
from influential physicians will be essential for widespread market acceptance. Our product candidates are still in the development stage
and it is premature to attempt to gain support from physicians at this time. We can provide no assurance that such support will ever be
obtained. If our product candidates do not receive such support from these physicians and from long-term data, physicians may not use
or continue to use, and hospitals may not purchase or continue to purchase, them.
Failure of Iomab-B, Actimab-A
or any of our other product candidates to significantly penetrate current or new markets would negatively impact our business financial
condition and results of operations.
We may be subject to claims that our third-party
service providers, consultants or current or former employees have wrongfully used or disclosed confidential information of third parties.
We have received confidential
and proprietary information from third parties. In addition, we employ individuals who were previously employed at other biotechnology
or pharmaceutical companies. We may be subject to claims that we or our employees, consultants or independent contractors have inadvertently
or otherwise used or disclosed confidential information of these third parties or our employees’ former employers. Litigation may
be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial
cost and be a distraction to our management and employees.
We currently depend on single third-party
manufacturers to produce our pre-clinical and clinical trial drug supplies. Any disruption in the operations of our current third-party
manufacturers, or other third-party manufacturers we may engage in the future, could adversely affect our business and results of operations.
We do not currently operate
manufacturing facilities for pre-clinical or clinical production of any of our product candidates. We rely on third-party manufacturers
to supply, store, and distribute pre-clinical and clinical supply of the components of our drug product candidates including monoclonal
antibodies, linkers and radioisotopes, as well as the final construct which comprises our drug product candidates. We expect to continue
to depend on third-party manufacturers for the foreseeable future. Any performance failure on the part of our existing or future manufacturers
could delay clinical development, cause us to suspend or terminate development or delay or prohibit regulatory approval of our product
candidates or commercialization of any approved products. Further avenues of disruption to our clinical or eventual commercial supply
may also occur due to the sale, acquisition, business reprioritization, bankruptcy or other unforeseen circumstances that might occur
at any of our suppliers or contract manufacturing partners including an inability to come to terms on renewal of existing contracts or
new contracts.
We currently rely on single
manufacturers to manufacture our pre-clinical and clinical trial drug supplies. With a view to maintaining business continuity we are
evaluating alternatives and second and even third sources of supply or manufacturing for our core suppliers and manufacturing partners,
however there can be no assurances that we will be able to identify such suppliers or partners and assuming we did, that we would be able
to enter into contracts that are on favorable terms or on terms that will enable sufficient supply to ensure business continuity and support
our growth plans.
Our product candidates require
precise, high-quality manufacturing. Failure by our current contract manufacturer or other third-party manufacturers we may engage in
the future to achieve and maintain high manufacturing standards could result in patient injury or death, product recalls or withdrawals,
delays or failures in testing or delivery, cost overruns, or other problems that could seriously hurt our business. Contract manufacturers
may encounter difficulties involving production yields, quality control, and quality assurance. These manufacturers are subject to ongoing
periodic and unannounced inspections by the FDA and corresponding state and foreign agencies to ensure strict compliance with cGMPs and
other applicable government regulations and corresponding foreign standards; we do not have control over third-party manufacturers’
compliance with these regulations and standards.
We may elect to build or purchase
a manufacturing facility or facilities in the future to operate for the purposes of manufacturing our own products. We have never built,
owned or operated a manufacturing facility. There can be no assurances that we will be able to successfully accomplish this and in doing
so we may experience delays, cost overruns, or other problems that could seriously hurt our business. Even if we successfully build or
purchase a manufacturing facility, we may not realize the expected benefits of these efforts.
We depend on vendors with
specialized operations, equipment and know-how to manufacture the respective components of our drug candidates. We have entered into manufacturing
and supply agreements with these third-parties, and in some instances, we have agreed that such vendor be the exclusive manufacturer and
supplier. If any of the third-parties we depend on encounter difficulties in their operations, fail to comply with required regulations
or breach their contractual obligations it may be difficult, or we may be unable to identify suitable alternative third-party manufacturers.
While we identify and evaluate third-party manufacturers from time to time, even if we do identify suitable alternative third-parties,
we may fail to reach agreement on contractual terms, it may be prohibitively expensive and there can be no assurance that we can successfully
complete technology transfer and development work necessary or complete the necessary work in a timely manner. Any of which could prevent
us from commencing manufacturing with third-parties which could cause delays or suspension of our clinical trials and pre-clinical work
that may have a negative impact on our business.
Furthermore, these third-party
contractors, whether foreign or domestic, may experience regulatory compliance difficulty, mechanical shutdowns, employee strikes, or
any other unforeseeable acts that may delay or limit production. Our inability to adequately establish, supervise and conduct (either
ourselves or through third parties) all aspects of the formulation and manufacturing processes, and the inability of third-party manufacturers
to consistently supply quality product when required would have a material adverse effect on our ability to develop or commercialize our
products. We have faced delays and risks associated with reliance on key third party manufacturers in the past and may be faced with such
delays and risks in the future. Any future manufacturing interruptions or related supply issues could have an adverse effect on our company,
including delays in clinical trials.
If we are successful in obtaining marketing
approval from the FDA and/or other regulatory agencies for any of our product candidates, we anticipate continued reliance on third-party
manufacturers.
To date, our product candidates
have been manufactured in small quantities for preclinical and clinical testing by third-party manufacturers. If the FDA or other regulatory
agencies approve any of our product candidates for commercial sale, we expect that we would continue to rely, at least initially, on third-party
specialized manufacturers to produce commercial quantities of approved products. These manufacturers may not be able to successfully increase
the manufacturing capacity for any approved product in a timely or economic manner, or at all. Significant scale-up of manufacturing may
require additional validation studies, which the FDA must review and approve. Scale-up for commercial product may require financial commitment
or investment by us, which we may not have sufficient capital for or may elect not to undertake. If third party manufacturers are unable
to successfully increase the manufacturing capacity for a product candidate, or we are unable to establish our own manufacturing capabilities,
the commercial launch of any approved products may be delayed or there may be a shortage in supply, which in turn could have a material
adverse effect on our business.
In addition, the facilities
used by our contract manufacturers to manufacture our product candidates must be approved by the FDA pursuant to inspections that will
be conducted after we submit a BLA to the FDA. We do not control the manufacturing process of, and are completely dependent on, our contract
manufacturing partners for compliance with cGMPs. If our contract manufacturers cannot successfully manufacture material that conforms
to our specifications and the strict regulatory requirements of the FDA or other regulatory authorities, they will not be able to secure
and/or maintain regulatory approval for their manufacturing facilities. If the FDA or a comparable foreign regulatory authority does not
approve these facilities for the manufacture of our product candidates or if it withdraws any such approval in the future, we may need
to find alternative manufacturing facilities, which would significantly impact our ability to develop, obtain regulatory approval for
or market our product candidates, if approved.
We may have conflicts with our partners
that could delay or prevent the development or commercialization of our product candidates.
We may have conflicts with
our partners, such as conflicts concerning the interpretation of preclinical or clinical data, the achievement of milestones, the interpretation
of contractual obligations, payments for services, development obligations or the ownership of intellectual property developed during
our collaboration. If any conflicts arise with any of our partners, such partner may act in a manner that is adverse to our best interests.
Any such disagreement could result in one or more of the following, each of which could delay or prevent the development or commercialization
of our product candidates, and in turn prevent us from generating revenues: unwillingness on the part of a partner to pay us milestone
payments or royalties we believe are due under a collaboration; uncertainty regarding ownership of intellectual property rights arising
from our collaborative activities, which could prevent us from entering into additional collaborations; unwillingness by the partner to
cooperate in the development or manufacture of the product, including providing us with product data or materials; unwillingness on the
part of a partner to keep us informed regarding the progress of its development and commercialization activities or to permit public disclosure
of the results of those activities; initiating litigation or alternative dispute resolution options by either party to resolve the dispute;
or attempts by either party to terminate the agreement.
If in the future we are unable to establish
U.S. or global sales and marketing capabilities or enter into agreements with third parties to sell and market our product candidates,
we may not be successful in commercializing our product candidates if they are approved and we may not be able to generate any revenue.
We currently do not have a
marketing or sales team for the marketing, sales and distribution of any of our product candidates that may receive regulatory approval.
In order to commercialize any product candidates after approval, we must build on a territory-by-territory basis marketing, sales, distribution,
managerial and other non-technical capabilities or make arrangements with third parties to perform these services, and we may not be successful
in doing so. If our product candidates receive regulatory approval, we may decide to establish an internal sales or marketing team with
technical expertise and supporting distribution capabilities to commercialize our product candidates, which will be expensive and time-consuming
and will require significant attention of our executive officers to manage. Any failure or delay in the development of our internal sales,
marketing and distribution capabilities would adversely impact the commercialization of any of our product candidates that we obtain approval
to market.
With respect to the commercialization
of all or certain of our product candidates, we may choose to collaborate, either globally or on a territory-by-territory basis, with
third parties that have direct sales forces and established distribution systems, either to augment our own sales force and distribution
systems or in lieu of our own sales force and distribution systems. In particular, we have and expect to continue to partner with third
parties to commercialize Iomab-B outside the United States. In April 2022, we entered into a licensing agreement with Immedica, in
which Immedica acquired the product rights for commercialization of Iomab-B for certain territories outside the U.S. If we are unable
to enter into or maintain such arrangements when needed on acceptable terms, or at all, we may not be able to successfully commercialize
any of our product candidates that receive regulatory approval or any such commercialization may experience delays or limitations. If
we are not successful in commercializing our product candidates, either on our own or through collaborations with one or more third parties,
our future product revenue will suffer and we may incur significant additional losses.
We face significant competition from other
biotechnology and pharmaceutical companies.
Our product candidates face,
and will continue to face, intense competition from large pharmaceutical and biotechnology companies, as well as academic and research
institutions. We compete in an industry that is characterized by (i) rapid technological change, (ii) evolving industry standards, (iii)
emerging competition and (iv) new product introductions. Our competitors have existing products and technologies that will compete with
our product candidates and technologies and may develop and commercialize additional products and technologies that will compete with
our product candidates and technologies. Because several competing companies and institutions have greater financial resources than us,
they may be able to (i) provide broader services and product lines, (ii) make greater investments in research and development, or R&D,
and (iii) carry on broader R&D initiatives. Our competitors also have greater development capabilities than we do and have substantially
greater experience in undertaking preclinical and clinical testing of product candidates, obtaining regulatory approvals, and manufacturing
and marketing pharmaceutical products. They also have greater name recognition and better access to customers than us.
Our product candidates may cause undesirable
side effects or have other properties that could halt their clinical development, prevent their regulatory approval, limit their commercial
potential, or result in significant negative consequences.
Undesirable side effects caused
by our product candidates could cause us or regulatory authorities to interrupt, delay or halt clinical trials and could result in a more
restrictive label or the delay or denial of regulatory approval by the FDA or other comparable foreign authorities. The drug-related side
effects could affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability
claims. Any of these occurrences may harm our business, financial condition and prospects significantly. Even if any of our product candidates
receives marketing approval, as greater numbers of patients use a product following its approval, an increase in the incidence of side
effects or the incidence of other post-approval problems that were not seen or anticipated during pre-approval clinical trials could result
in a number of potentially significant negative consequences, including:
| |
● |
regulatory authorities may withdraw their approval of the product; |
| |
● |
regulatory authorities may require the addition of labeling statements, such as warnings or contraindications; |
| |
● |
we may be required to change the way the product is administered, conduct additional clinical trials or change the labeling of the product; |
| |
● |
we may elect, or we may be required, to recall or withdraw product from the market; |
| |
● |
we could be sued and held liable for harm caused to patients; and |
| |
● |
our reputation may suffer. |
Any of these events could
substantially increase the costs and expenses of developing, commercializing and marketing any such product candidates or could harm or
prevent sales of any approved products.
Risks Related to Our Intellectual Property
We depend upon securing and protecting critical
intellectual property.
We are dependent on obtaining
and maintaining patents, trade secrets, copyright and trademark protection of our technologies in the United States and other jurisdictions,
as well as successfully enforcing this intellectual property and defending this intellectual property against third-party challenges.
The degree of future protection of our proprietary rights is uncertain for product candidates that are currently in the early stages of
development because we cannot predict which of these product candidates will ultimately reach the commercial market or whether the commercial
versions of these product candidates will incorporate proprietary technologies.
Our patent position is highly uncertain
and involves complex legal and factual questions.
Accordingly, we cannot predict
the breadth of claims that may be allowed or enforced under our patents or in third-party patents. For example, we or our licensors might
not have been the first to make the inventions covered by each of our pending patent applications and issued patents; we or our licensors
might not have been the first to file patent applications for these inventions; others may independently develop similar or alternative
technologies or duplicate any of our technologies; it is possible that none of our pending patent applications or the pending patent applications
of our licensors will result in issued patents; our issued patents and issued patents of our licensors may not provide a basis for commercially
viable technologies, or may not provide us with any competitive advantages, or may be challenged and invalidated by third parties; and,
we may not develop additional proprietary technologies that are patentable.
As a result, our owned and
licensed patents may not be valid, and we may not be able to obtain and enforce patents and to maintain trade secret protection for the
full commercial extent of our technology. The extent to which we are unable to do so could materially harm our business.
We or our licensors have applied
for and will continue to apply for patents for certain products and methods. Such applications may not result in the issuance of any patents,
and any patents now held or that may be issued may not provide us with adequate protection from competition. Furthermore, it is possible
that patents issued or licensed to us may be challenged successfully. In that event, if we have a preferred competitive position because
of such patents, such preferred position would be lost. If we are unable to secure or to continue to maintain a preferred position, we
could become subject to competition from the sale of generic products. Failure to receive, inability to protect, or expiration of our
patents for medical use, manufacture, conjugation and labeling of Ac-225, the antibodies that we license from third parties, or subsequent
related filings, would adversely affect our business and operations.
Patents issued or licensed
to us may be infringed by the products or processes of others. The cost of enforcing our patent rights against infringers, if such enforcement
is required, could be significant, and we do not currently have the financial resources to fund such litigation. Further, such litigation
can go on for years and the time demands could interfere with our normal operations. There has been substantial litigation and other proceedings
regarding patent and other intellectual property rights in the pharmaceutical industry. We may become a party to patent litigation and
other proceedings. The cost to us of any patent litigation, even if resolved in our favor, could be substantial. Some of our competitors
may be able to sustain the costs of such litigation more effectively than we can because of their substantially greater financial resources.
Litigation may also absorb significant management time.
Unpatented trade secrets,
improvements, confidential know-how and continuing technological innovation are important to our scientific and commercial success. Although
we attempt to and will continue to attempt to protect our proprietary information through reliance on trade secret laws and the use of
confidentiality agreements with our partners, collaborators, employees and consultants and other appropriate means, these measures may
not effectively prevent disclosure of our proprietary information, and, in any event, others may develop independently, or obtain access
to, the same or similar information. In addition, we cannot guarantee that we have executed these agreements with each party that may
have or have had access to our trade secrets. Furthermore, if the employees and consultants who are parties to these agreements breach
or violate the terms of these agreements, we may not have adequate remedies for any such breach or violation, and we could lose our trade
secrets through such breaches or violations.
Certain of our patent rights
are licensed to us by third parties. If we fail to comply with the terms of these license agreements, our rights to those patents may
be terminated, and we may be unable to conduct our business.
If we are found to be infringing on patents
or trade secrets owned by others, we may be forced to cease or alter our product development efforts, obtain a license to continue the
development or sale of our products, and/or pay damages.
Our manufacturing processes
and potential products may violate proprietary rights of patents that have been or may be granted to competitors, universities or others,
or the trade secrets of those persons and entities. As the pharmaceutical industry expands and more patents are issued, the risk increases
that our processes and potential products may give rise to claims that they infringe the patents or trade secrets of others. These other
persons could bring legal actions against us claiming damages and seeking to enjoin clinical testing, manufacturing and marketing of the
affected product or process. If any of these actions are successful, in addition to any potential liability for damages, we could be required
to obtain a license in order to continue to conduct clinical tests, manufacture or market the affected product or use the affected process.
Required licenses may not be available on acceptable terms, if at all, and the results of litigation are uncertain. If we become involved
in litigation or other proceedings, it could consume a substantial portion of our financial resources and the efforts of our personnel.
In addition to infringement
or other intellectual property claims against us, we may become a party to other patent litigation or proceedings before regulatory agencies,
including post-grant review, inter parties review, interference or re-examination proceedings filed with the U.S. Patent and Trademark
Office (or similar proceedings before corresponding tribunals in other jurisdictions) that challenge our patent rights or the patent rights
of our licensors. The costs and efforts of defending our patents or enforcing our proprietary rights in post-issuance administrative proceedings
can be substantial and the outcome can be uncertain. An adverse determination in these proceedings could weaken or invalidate the patent
claims that cover our technology, which adverse determination could harm our business significantly and dissuade companies from collaborating
with us or permit third parties to directly compete with the same technology.
Our ability to protect and enforce our patents
does not guarantee that we will secure the right to commercialize our patents.
A patent is a limited monopoly
right conferred upon an inventor, and his successors in title, in return for the making and disclosing of a new and non-obvious invention.
This monopoly is of limited duration but, while in force, allows the patent holder to prevent others from making and/or using its invention.
While a patent gives the holder this right to exclude others, it is not a license to commercialize the invention where other permissions
may be required for commercialization to occur. For example, a drug cannot be marketed without the appropriate authorization from the
FDA, regardless of the existence of a patent covering the product. Further, the invention, even if patented itself, cannot be commercialized
if it infringes the valid patent rights of another party.
We rely on confidentiality agreements to
protect our trade secrets. If these agreements are breached by our employees or other parties, our trade secrets may become known to our
competitors.
We rely on trade secrets that
we seek to protect through numerous measures, including non-compete and confidentiality agreements with our employees and other parties.
If these agreements are breached, our competitors may obtain and use our trade secrets to gain a competitive advantage over us. Any remedies
that may be available to us may not be adequate to protect our business or compensate us for the damaging disclosure. In addition, we
may have to expend resources to protect our interests from possible infringement by others. For instance, we learned that a former employee,
Qing Liang, Ph.D., who was employed by Actinium in the position of Vice President, Head of Radiation Sciences, violated the non-compete
provision of her employment agreement by working for a direct competitor. Additionally, while working for the direct competitor, Dr. Liang
continued to provide consulting services to Actinium. We also learned that Dr. Liang was providing consulting services to another company,
which was in violation of certain provisions of her post-employment consulting agreement with Actinium. Dr. Liang, who had access to materials
containing proprietary information and trade secrets, pursuant to actions taken by Actinium, is no longer employed by the direct competitor.
With the assistance of outside counsel and a forensic investigator, we identified that Dr. Liang downloaded confidential information prior
to her employment at Actinium ending. To aid in arbitration proceedings, we petitioned and were granted a Stipulated Preliminary Injunction
by the Supreme Court of the State of New York, New York County (Index No. 656841/2022) on June 28, 2022 that ordered that Dr. Liang is
enjoined from destroying or deleting any Actinium documents or information, is enjoined from using, transmitting or transferring any Actinium
Information other than to her counsel or Actinium’s counsel, ordered to return Actinium information within 5 days of Stipulated
Preliminary Injunction, ordered to disclose to Actinium under oath, all persons and devices she transferred or disclosed Actinium Information,
and ordered to allow a qualified forensic examiner selected by Actinium to remove and permanently delete all Actinium Information from
any electronic devices, systems, email accounts, or other electronic or physical storage sites belonging to Dr. Liang. We are currently
in arbitration with Dr. Liang and intend to enforce the terms of her employment agreement, especially the non-compete and confidentiality
provisions, to the fullest extent of our ability. On April 25, 2023, a Final Award and Permanent Injunction was granted by the Supreme
Court of the State of New York, New York County (Case No. 01-22-0003-2375_ that ordered that Ms. Liang is permanently enjoined from using,
possessing, transmitting or transferring any Actinium property, documents of business information. Further, until April 1, 2024, Dr. Liang
shall not, either directly or indirectly, engage in any business that directly or indirectly is developing, or plans to develop, radioimmunotherapies
for cancer or any targeted conditioning therapy or agent for adoptive cell therapy including bone marrow transplant and CAR-T.
Risks Related to Our Operations
We expect to expand our development and
regulatory capabilities and potentially implement sales, marketing and distribution capabilities, and, as a result, we may encounter difficulties
in managing our growth, which could disrupt our operations.
We expect to experience significant
growth in the number of our employees and the scope of our operations, particularly in the areas of product candidate development, regulatory
affairs and, if any of our product candidates receives marketing approval, sales, marketing and distribution.
We currently do not have a
marketing or sales team for the marketing, sales and distribution of any of our product candidates that are potentially able to obtain
regulatory approval. In order to commercialize any product candidates, we must build on a territory-by-territory basis marketing, sales,
distribution, managerial and other non-technical capabilities or make arrangements with third parties to perform these services, and we
may not be successful in doing so. If our product candidates receive regulatory approval, we intend to establish an internal sales or
marketing team with technical expertise and supporting distribution capabilities to commercialize our product candidates, which will be
expensive and time consuming and will require significant attention of our executive officers to manage. We will also have to compete
with other pharmaceutical and biotechnology companies to recruit, hire, train and retain marketing and sales personnel. Any failure or
delay in the development of our internal sales, marketing and distribution capabilities would adversely impact the commercialization of
any of our product candidates that we obtain approval to market.
To manage our anticipated
future growth, we must continue to implement and improve our managerial, operational and financial systems, expand our facilities and
continue to recruit and train additional qualified personnel. Due to our limited financial resources and the limited experience of our
management team in managing a public company with such anticipated growth, we may not be able to effectively manage the expansion of our
operations or recruit and train additional qualified personnel. The expansion of our operations may lead to significant costs and may
divert our management and business development resources. Any inability to manage growth could delay the execution of our business plans
or disrupt our operations.
The use of hazardous materials, including
radioactive and biological materials, in our research and development efforts imposes certain compliance costs on us and may subject us
to liability for claims arising from the use or misuse of these materials.
Our research, development
and manufacturing activities involve the controlled use of hazardous materials, including chemicals, radioactive and biological materials,
such as radioactive isotopes. We are subject to federal, state, local and foreign environmental laws and regulations governing, among
other matters, the handling, storage, use and disposal of these materials and some waste products. We cannot completely eliminate the
risk of contamination or injury from these materials and we could be held liable for any damages that result, which could exceed our financial
resources. We currently maintain insurance coverage for injuries resulting from the hazardous materials we use; however, future claims
may exceed the amount of our coverage. Also, we do not have insurance coverage for pollution cleanup and removal. Currently the costs
of complying with such federal, state, local and foreign environmental regulations are not significant, and consist primarily of waste
disposal expenses. However, they could become expensive, and current or future environmental laws or regulations may impair our research,
development, production and commercialization efforts.
We may undertake international operations,
which will subject us to risks inherent with operations outside of the United States.
Although we do not have any
international operations at this time, we intend to seek market clearances in foreign markets that we believe will generate significant
opportunities. However, even with the cooperation of a commercialization partner, conducting drug development in foreign countries involves
inherent risks, including, but not limited to difficulties in staffing, funding and managing foreign operations; unexpected changes in
regulatory requirements; export restrictions; tariffs and other trade barriers; difficulties in protecting, acquiring, enforcing and litigating
intellectual property rights; fluctuations in currency exchange rates; and potentially adverse tax consequences.
If we were to experience any
of the difficulties listed above, or any other difficulties, any international development activities and our overall financial condition
may suffer and cause us to reduce or discontinue our international development and registration efforts.
We are highly dependent on our key personnel,
and if we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our
business strategy.
Our future operations and
successes depend in large part upon the continued service of key members of our senior management team whom we are highly dependent upon
to manage our business. If any member of our current senior management terminates his or her employment with us and we are unable to find
a suitable replacement quickly, the departure could have a material adverse effect on our business. An overall tightening and increasingly
competitive labor market has been observed in the U.S. employment market generally, especially in response to the COVID-19 pandemic. Specific
to the biotechnology industry in which we operate, there is significant demand and competition for highly specialized talent that we require.
A sustained labor shortage or increased turnover rates within our employee base, caused by the COVID-19 pandemic, as a result of general
macroeconomic factors, or due to dynamics within our industry, could lead to increased costs, such as increased wage rates to attract
and retain employees, and could negatively affect our ability to efficiently conduct our clinical development, R&D, business development
and potential regulatory and commercial activities. If we are unable to hire and retain employees capable of performing at a high-level,
or if mitigation measures we may take to respond to a decrease in labor availability, have unintended negative effects, our business could
be adversely affected. An overall labor shortage, lack of skilled labor, increased turnover or labor inflation, caused by the COVID-19
pandemic, general macroeconomic factors or as a result of biotechnology industry dynamics could have a material adverse impact on our
operations, results of operations, liquidity or cash flows.
Our future success also depends
on our ability to identify, attract, hire or engage, retain and motivate other well-qualified managerial, technical, clinical and regulatory
personnel. This activity is likely to create additional demands on the time and attention of our senior management personnel as they identify,
hire, and train external and internal candidates to fill the sizable number of positions required to execute our business plans, including
submitting a BLA and building a commercial organization. The market for talent in our industry is very competitive. Many of the other
biopharmaceutical companies we compete against for qualified personnel have greater financial and other resources, more favorable risk
profiles and a longer operating history in the biopharmaceutical industry than we do. They also may provide more diverse opportunities
and better chances for career advancement. Some of these opportunities may be more appealing to high-quality candidates than what we have
to offer. There can be no assurance that such professionals will be available in the market, or that we will be able to retain existing
professionals or meet or continue to meet their compensation requirements. Furthermore, the cost base in relation to such compensation,
which may include equity compensation, may increase significantly, which could have a material adverse effect on us. Failure to establish
and maintain an effective management team and workforce could adversely affect our ability to operate, grow and manage our business.
Managing our growth as we expand operations
may strain our resources.
We expect to need to grow
rapidly in order to support additional, larger, and potentially international, pivotal clinical trials of our product candidates as well
as potential commercial operations, which will place a significant strain on our financial, managerial and operational resources. In order
to achieve and manage growth effectively, we must continue to improve and expand our operational and financial management capabilities.
Moreover, we will need to increase staffing and to train, motivate and manage our employees. All of these activities will increase our
expenses and may require us to raise additional capital sooner than expected. Failure to manage growth effectively could materially harm
our business, financial condition or results of operations.
We may expand our business through the acquisition
of rights to new product candidates that could disrupt our business, harm our financial condition and may also dilute current stockholders’
ownership interests in our company.
Our business strategy includes
expanding our products and capabilities, and we may seek acquisitions of product candidates, antibodies or technologies to do so. Acquisitions
involve numerous risks, including substantial cash expenditures; potentially dilutive issuance of equity securities; incurrence of debt
and contingent liabilities, some of which may be difficult or impossible to identify at the time of acquisition; difficulties in assimilating
acquired technologies or the operations of the acquired companies; diverting our management’s attention away from other business
concerns; risks of entering markets in which we have limited or no direct experience; and the potential loss of our key employees or key
employees of the acquired companies.
We can make no assurances
that any acquisition will result in short-term or long-term benefits to us. We may incorrectly judge the value or worth of an acquired
product, company or business. In addition, our future success would depend in part on our ability to manage the rapid growth associated
with some of these acquisitions. We cannot assure that we will be able to make the combination of our business with that of acquired products,
businesses or companies work or be successful. Furthermore, the development or expansion of our business or any acquired products, business
or companies may require a substantial capital investment by us. We may not have these necessary funds, or they might not be available
to us on acceptable terms or at all. We may also seek to raise funds by selling shares of our preferred or common stock, which could dilute
each current stockholder’s ownership interest in the Company.
Risks Related to Ownership of Our Common Stock
The sale of securities by us in any equity
or debt financing could result in dilution to our existing stockholders and have a material adverse effect on our earnings.
We have financed our operations
primarily through sales of stock and warrants. It is likely that during the next twelve months we will seek to raise additional capital
through the sales of stock and warrants in order to expand our level of operations to continue our research and development efforts.
Any sale of common stock by
us in a future offering could result in dilution to our existing stockholders as a direct result of our issuance of additional shares
of our capital stock. In addition, our business strategy may include expansion through internal growth or by establishing strategic relationships
with targeted customers and vendors. In order to do so, or to finance the cost of our other activities, we may issue additional equity
securities that could dilute our stockholders’ stock ownership. We may also assume additional debt and incur impairment losses related
to goodwill and other tangible assets if we acquire another company and this could negatively impact our earnings and results of operations.
Our common stock is subject to price volatility which could
lead to losses by stockholders and potential costly security litigation.
The trading volume of our
common stock has been and may continue to be extremely limited and sporadic. We expect the market price of our common stock to fluctuate
substantially due to a variety of factors, including market perception of our ability to achieve our planned growth, quarterly operating
results of other companies in the same industry, trading volume in our common stock, changes in general conditions in the economy and
the financial markets or other developments affecting our competitors or us. This volatility has had a significant effect on the market
price of securities issued by many companies for reasons unrelated to their operating performance and could have the same effect on our
common stock.
The trading price of our common
stock may be highly volatile and could fluctuate in response to factors such as:
| |
● |
actual or anticipated variations in our operating results; |
| |
● |
announcements of developments by us or our competitors; |
| |
● |
the timing of IND and/or BLA approval, the completion and/or results of our clinical trials; |
| |
● |
regulatory actions regarding our products; |
| |
● |
announcements by us or our competitors of significant acquisitions, strategic partnerships, joint ventures or capital commitments; |
| |
● |
adoption of new accounting standards affecting our industry; |
| |
● |
additions or departures of key personnel; |
| |
● |
introduction of new products by us or our competitors; |
| |
● |
sales of our common stock or other securities in the open market; |
| |
● |
inaccurate or unfavorable reports from securities or industry analysts; and |
| |
● |
other events or factors, many of which are beyond our control. |
The stock market is subject
to significant price and volume fluctuations. In the past, following periods of volatility in the market price of a company’s securities,
securities class action litigation has often been initiated against such a company. Litigation initiated against us, whether or not successful,
could result in substantial costs and diversion of our management’s attention and our resources, which could harm our business and
financial condition.
We do not intend to pay dividends on our
common stock, so any returns will be determined by the value of our common stock.
We have never declared or
paid any cash dividends on our common stock. For the foreseeable future, it is expected that earnings, if any, generated from our operations
will be used to finance the growth of our business, and that no dividends will be paid to holders of our common stock. As a result, the
success of an investment in our common stock will depend upon any future appreciation in its value. There is no guarantee that our common
stock will appreciate in value.
Certain provisions of our Certificate
of Incorporation and Bylaws and Delaware law make it more difficult for a third party to acquire us and make a takeover more difficult
to complete, even if such a transaction were in our stockholders’ interest.
Provisions of our certificate
of incorporation and bylaws may delay or discourage transactions involving an actual or potential change in our control or change in our
management, including transactions in which stockholders might otherwise receive a premium for their shares, or transactions that our
stockholders might otherwise deem to be in their best interests. Therefore, these provisions could adversely affect the price of our stock.
Among other things, the certificate of incorporation and bylaws:
| |
● |
provide that the authorized number of directors may be changed by resolution of the board of directors; |
| |
● |
provide that all vacancies, including newly-created directorships, may, except as otherwise required by law, be filled by the affirmative vote of a majority of directors then in office, even if less than a quorum; |
| |
● |
divide the board of directors into three classes; |
| |
● |
provide that stockholders seeking to present proposals before a meeting of stockholders or to nominate candidates for election as directors at a meeting of stockholders must provide notice in writing in a timely manner, and meet specific requirements as to the form and content of a stockholder’s notice; |
In addition, we are governed
by Section 203 of the Delaware General Corporation Law. In general, Section 203 prohibits a public Delaware corporation from engaging
in a “business combination” with an “interested stockholder” for a period of three years after the date of the
transaction in which the person became an interested stockholder, unless the business combination is approved in a prescribed manner.
A “business combination” includes mergers, asset sales or other transactions resulting in a financial benefit to the stockholder.
An “interested stockholder” is a person who, together with affiliates and associates, owns, or within three years, did own,
15% or more of the corporation’s outstanding voting stock. These provisions may have the effect of delaying, deferring or preventing
a change in our control.
General Risk Factors
Compliance with the reporting requirements
of federal securities laws can be expensive.
We are subject to the information
and reporting requirements of the Exchange Act and other federal securities laws, and the compliance obligations of the Sarbanes-Oxley
Act. The costs of preparing and filing annual and quarterly reports and other information with the Securities and Exchange Commission
and furnishing audited reports to stockholders are substantial. In addition, we will incur substantial expenses in connection with the
preparation of registration statements and related documents with respect to any offerings of our common stock.
Our ability to utilize our net operating
loss carryforwards and certain other tax attributes may be limited.
Our ability to utilize our
federal net operating loss and tax credit carryforwards may be limited under Sections 382 and 383 of the Internal Revenue Code of 1986,
as amended, or the Code. The limitations apply if we experience an “ownership change”, generally defined as a greater
than 50 percentage point change in the ownership of our equity by certain stockholders over a rolling three-year period. Similar
provisions of state tax law may also apply. We have not assessed whether such an ownership change has previously occurred. If we
have experienced an ownership change at any time since our formation, we may already be subject to limitations on our ability to utilize
our existing net operating losses and other tax attributes to offset taxable income. In addition, future changes in our stock ownership,
which may be outside of our control, may trigger an ownership change and, consequently, the limitations under Sections 382 and 383 of
the Code. As a result, if or when we earn net taxable income, our ability to use our pre-change net operating loss carryforwards
and other tax attributes to offset such taxable income may be subject to limitations, which could adversely affect our future cash flows.
Failure to establish and maintain adequate
finance infrastructure and accounting systems and controls could impair our ability to comply with the financial reporting and internal
controls requirements for publicly traded companies.
As a public company, we operate
in an increasingly demanding regulatory environment, including with respect to more complex accounting rules. Company responsibilities
required by the Sarbanes-Oxley Act of 2002, as amended, or the Sarbanes-Oxley Act, include establishing and maintaining corporate oversight
and adequate internal control over financial reporting and disclosure controls and procedures. Effective internal controls are necessary
for us to produce reliable financial reports and are important to help prevent financial fraud.
Our compliance with Section
404 of the Sarbanes-Oxley Act requires that we incur substantial accounting expense and expend significant management efforts. We complied
with Section 404 at December 31, 2022 and 2021 and while our testing did not reveal any material weaknesses in our internal controls,
any material weaknesses in our internal controls in the future would be required us to remediate in a timely manner so as to be able to
comply with the requirements of Section 404 each year. If we are not able to comply with the requirements of Section 404 in a timely manner
each year, we could be subject to sanctions or investigations by the SEC, NYSE American or other regulatory authorities which would require
additional financial and management resources and could adversely affect the market price of our common stock. Furthermore, if we cannot
provide reliable financial reports or prevent fraud, our business and results of operations could be harmed, and investors could lose
confidence in our reported financial information.
If securities or industry analysts do not
publish research or publish inaccurate or unfavorable research about our business, the price of our common stock and trading volume could
decline.
The trading market for our
common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. Multiple
securities and industry analysts currently cover us. If one or more of the analysts downgrade our common stock or publish inaccurate or
unfavorable research about our business, the price of our common stock would likely decline. If one or more of these analysts cease coverage
of us or fail to publish reports on us regularly, demand for our common stock could decrease, which could cause the price of our common
stock and trading volume to decline.
Our amended and restated bylaws, as
amended, designate the U.S. federal district courts as the exclusive forum for the resolution of any complaint
asserting a cause of action arising under the Securities Act of 1933, as amended.
Our amended and restated bylaws,
as amended, provide that, unless we consent in writing to the selection of an alternative forum, the federal district courts of the
United States of America will be the exclusive forum for resolving any complaint asserting a cause of action arising under the Securities
Act of 1933, as amended. In addition, our amended and restated bylaws, as amended, state that any person purchasing or otherwise acquiring
any interest in our security shall be deemed to have notice of and to have consented to such provision. Such choice of forum provision
may limit a stockholder’s ability to bring a claim in a judicial forum that it finds favorable for disputes with us or our directors,
officers or other employees, which may discourage such lawsuits, if successful, might benefit our stockholders. Stockholders who do bring
a claim in the federal district courts of the United States of America could face additional litigation costs in pursuing any such claim.
ITEM 2. UNREGISTERED SALES OF EQUITY SECURITIES AND USE OF PROCEEDS.
None.
ITEM 3. DEFAULTS UPON SENIOR SECURITIES.
None.
ITEM 4. MINE SAFETY DISCLOSURES.
None.
ITEM 5. OTHER INFORMATION.
On November 1, 2023, the board of directors approved an amendment to the
employment agreement of the Company’s Chief Executive Officer and Chairman of the board of directors, Sandesh Seth, pursuant to
which the term of Mr. Seth’s employment was extended from February 21, 2024 to February 21, 2027, subject to the terms of the employment
agreement.
ITEM 6. EXHIBITS
Copies of the following documents
are included as exhibits to this report pursuant to Item 601 of Regulation S-K.
| Exhibit No. |
|
Description |
| 3.1 |
|
Certificate of Incorporation of Actinium Pharmaceuticals, Inc. (incorporated by reference to Exhibit 3.1 of the Company’s Form 8-K filed with the SEC on April 17, 2013). |
| |
|
|
| 3.2 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed January 7, 2014 (incorporated by reference to Exhibit 3.5 to Form S-1 filed on January 31, 2014). |
| |
|
|
| 3.3 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed February 3, 2014. (incorporated by reference to Exhibit 3.1 to Form 8-K filed on February 7, 2014). |
| |
|
|
| 3.4 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed on February 26, 2015 (incorporated by reference to Exhibit 3.1 to Form 8-K filed on March 4, 2015). |
| |
|
|
| 3.5 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed on February 26, 2018 (incorporated by reference to Exhibit 3.1 to Form 8-K filed on February 26, 2018). |
| |
|
|
| 3.6 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed on March 6, 2019 (incorporated by reference to Exhibit 3.7 to Form 10-K filed on March 15, 2019). |
| |
|
|
| 3.7 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed on June 16, 2020 (incorporated by reference to Exhibit 3.1 to Form 8-K filed on June 16, 2020). |
| |
|
|
| 3.8 |
|
Certificate of Amendment to Certificate of Incorporation, as amended, filed on August 10, 2020 (incorporated by reference to Exhibit 3.1 to Form 8-K filed on August 14, 2020). |
| |
|
|
| 3.9 |
|
Amended and Restated Bylaws, dated August 8, 2018 (incorporated by reference to Exhibit 3.1 to Form 10-Q filed on August 9, 2018). |
| |
|
|
| 3.10 |
|
Amendment to Amended and Restated Bylaws, dated May 7, 2020 (incorporated by reference to Exhibit 3.1 to Form 8-K filed on May 5, 2020). |
| |
|
|
| 10.1#* |
|
Amendment to Employment Agreement, dated November 1, 2023, by and between Actinium Pharmaceuticals, Inc. and Sandesh Seth. |
| # | Indicates
a management contract or compensatory plan or arrangement. |
SIGNATURES
Pursuant to the requirements
of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto
duly authorized.
| |
ACTINIUM PHARMACEUTICALS, INC. |
| |
|
|
| Date: November 2, 2023 |
By: |
/s/ Sandesh Seth |
| |
|
Sandesh Seth |
| |
|
Chairman and Chief Executive Officer
(Duly Authorized Officer and
Principal Executive Officer) |
| |
|
|
| |
By: |
/s/ Steve O’Loughlin |
| |
|
Steve O’Loughlin |
| |
|
Chief Financial Officer |
| |
|
(Duly Authorized Officer and
Principal Financial and Accounting Officer) |
74
0.38
0.49
0.94
1.50
23691218
25164599
26329298
27058397
false
--12-31
Q3
0001388320
0001388320
2023-01-01
2023-09-30
0001388320
2023-11-01
0001388320
2023-09-30
0001388320
2022-12-31
0001388320
2023-07-01
2023-09-30
0001388320
2022-07-01
2022-09-30
0001388320
2022-01-01
2022-09-30
0001388320
us-gaap:CommonStockMember
2022-12-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-12-31
0001388320
us-gaap:RetainedEarningsMember
2022-12-31
0001388320
us-gaap:CommonStockMember
2023-01-01
2023-03-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-01-01
2023-03-31
0001388320
us-gaap:RetainedEarningsMember
2023-01-01
2023-03-31
0001388320
2023-01-01
2023-03-31
0001388320
us-gaap:CommonStockMember
2023-03-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-03-31
0001388320
us-gaap:RetainedEarningsMember
2023-03-31
0001388320
2023-03-31
0001388320
us-gaap:CommonStockMember
2023-04-01
2023-06-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-04-01
2023-06-30
0001388320
us-gaap:RetainedEarningsMember
2023-04-01
2023-06-30
0001388320
2023-04-01
2023-06-30
0001388320
us-gaap:CommonStockMember
2023-06-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-06-30
0001388320
us-gaap:RetainedEarningsMember
2023-06-30
0001388320
2023-06-30
0001388320
us-gaap:CommonStockMember
2023-07-01
2023-09-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-07-01
2023-09-30
0001388320
us-gaap:RetainedEarningsMember
2023-07-01
2023-09-30
0001388320
us-gaap:CommonStockMember
2023-09-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2023-09-30
0001388320
us-gaap:RetainedEarningsMember
2023-09-30
0001388320
us-gaap:CommonStockMember
2021-12-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2021-12-31
0001388320
us-gaap:RetainedEarningsMember
2021-12-31
0001388320
2021-12-31
0001388320
us-gaap:CommonStockMember
2022-01-01
2022-03-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-01-01
2022-03-31
0001388320
us-gaap:RetainedEarningsMember
2022-01-01
2022-03-31
0001388320
2022-01-01
2022-03-31
0001388320
us-gaap:CommonStockMember
2022-03-31
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-03-31
0001388320
us-gaap:RetainedEarningsMember
2022-03-31
0001388320
2022-03-31
0001388320
us-gaap:CommonStockMember
2022-04-01
2022-06-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-04-01
2022-06-30
0001388320
us-gaap:RetainedEarningsMember
2022-04-01
2022-06-30
0001388320
2022-04-01
2022-06-30
0001388320
us-gaap:CommonStockMember
2022-06-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-06-30
0001388320
us-gaap:RetainedEarningsMember
2022-06-30
0001388320
2022-06-30
0001388320
us-gaap:CommonStockMember
2022-07-01
2022-09-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-07-01
2022-09-30
0001388320
us-gaap:RetainedEarningsMember
2022-07-01
2022-09-30
0001388320
us-gaap:CommonStockMember
2022-09-30
0001388320
us-gaap:AdditionalPaidInCapitalMember
2022-09-30
0001388320
us-gaap:RetainedEarningsMember
2022-09-30
0001388320
2022-09-30
0001388320
us-gaap:EmployeeStockOptionMember
2023-01-01
2023-09-30
0001388320
us-gaap:EmployeeStockOptionMember
2022-01-01
2022-09-30
0001388320
us-gaap:RestrictedStockUnitsRSUMember
2023-01-01
2023-09-30
0001388320
us-gaap:RestrictedStockUnitsRSUMember
2022-01-01
2022-09-30
0001388320
us-gaap:WarrantMember
2023-01-01
2023-09-30
0001388320
us-gaap:WarrantMember
2022-01-01
2022-09-30
0001388320
2012-06-15
0001388320
us-gaap:CorporateAndOtherMember
2023-09-30
0001388320
2008-12-31
0001388320
2022-05-31
0001388320
us-gaap:LicenseMember
2023-09-30
0001388320
us-gaap:LicenseMember
2022-12-31
0001388320
atnm:CapitalOnDemandSalesAgreementMember
2020-08-03
2020-08-31
0001388320
atnm:CapitalOnDemandSalesAgreementMember
2023-01-01
2023-09-30
0001388320
atnm:CapitalOnDemandSalesAgreementMember
2022-01-01
2022-09-30
0001388320
us-gaap:StockOptionMember
2023-01-01
2023-09-30
0001388320
srt:MinimumMember
2023-01-01
2023-09-30
0001388320
srt:MaximumMember
2023-01-01
2023-09-30
0001388320
us-gaap:StockOptionMember
2023-09-30
0001388320
us-gaap:StockOptionMember
2022-01-01
2022-09-30
0001388320
us-gaap:RestrictedStockUnitsRSUMember
2023-09-30
0001388320
us-gaap:RestrictedStockUnitsRSUMember
2023-01-01
2023-09-30
0001388320
us-gaap:RestrictedStockUnitsRSUMember
2022-01-01
2022-09-30
0001388320
2022-12-30
0001388320
2022-12-31
2022-12-31
0001388320
us-gaap:WarrantMember
2022-12-30
0001388320
us-gaap:WarrantMember
2022-12-31
2022-12-31
0001388320
us-gaap:WarrantMember
2023-01-01
2023-09-30
0001388320
us-gaap:WarrantMember
2023-09-30
xbrli:shares
iso4217:USD
iso4217:USD
xbrli:shares
xbrli:pure
1. Section
2(b) Performance Bonus of the Agreement is hereby amended as of the Amendment Effective Date by deleting the last sentence of said
section in its entirety and replacing it with the following new sentence:
Any such bonus shall be paid to you in the
calendar year following the annual period for which the bonus relates, and the Board shall make its best efforts to determine, award,
and have the Company pay out such bonus to you, if applicable, in the first calendar quarter of such calendar year.
2. Section
5 Term and Severance of the Agreement is hereby amended as of the Amendment Effective Date by deleting the date of “February
21, 2024” and substituting in lieu thereof the date “February 21, 2027”.
3. Section
5(d) “Good Reason” of the Agreement is hereby amended as of the Amendment Effective Date by deleting clause (vii) of
said section in its entirety and replacing it with the following new clause (vii):
(vii) the Company’s regular requirement
that you perform services in or relocate to a location that is more than 25 miles outside of New York City.
4. EXHIBIT
A RELEASE OF CLAIMS of the Agreement is hereby amended as of the Amendment Effective Date by deleting the date of “August 12,
2020” and substituting in lieu thereof the date of “November 1, 2023”.
5. Except
as expressly amended by this Amendment, the Agreement shall continue in full force and effect in accordance with the provisions thereof.
6. In
the event of a conflict between the Agreement and this Amendment, this Amendment shall govern.
18 U.S.C. SECTION 1350,
18 U.S.C. SECTION 1350,
18 U.S.C. SECTION 1350,
In connection with the Quarterly Report of Actinium Pharmaceuticals,
Inc. (the “Company”) on Form 10-Q for the period ended September 30, 2023 as filed with the Securities and Exchange Commission
on the date hereof (the “Report”), I, Sandesh Seth, Chairman & CEO of the Company, certify, pursuant to 18 U.S.C. Section
1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, that:
18 U.S.C. SECTION 1350,
In connection with the Quarterly Report of Actinium Pharmaceuticals,
Inc. (the “Company”) on Form 10-Q for the period ended September 30, 2023 as filed with the Securities and Exchange Commission
on the date hereof (the “Report”), I, Steve O’Loughlin, Chief Financial Officer of the Company, certify, pursuant to
18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, that: